
How to lose weight
Our conventional ideas about weight loss – eat less, move more – require a lot of willpower. Counting calories, exercising for hours every day and trying to ignore your hunger? At DietDoctor, we believe that’s needless suffering, and likely a waste of your time and precious energy.
Eventually people often give up. An excessive focus on counting calories has certainly not done much to reverse our current obesity epidemic.1 Fortunately there may be a better way.
The bottom line? Calories are not the only things that count in weight loss. Your weight is also hormonally regulated. If you reduce your hunger and the levels of hunger and fat-storing hormones you’ll likely have an easier time losing excess weight.2
Top 18 weight loss tips
Are you ready? Here we go. Start at the top of the list (most important) and go down as far as you need. Click on any tip to read all about it. Perhaps you only need the first piece of advice?
- Choose a low-carb or high satiety diet
- Eat when hungry
- Eat real food
- Eat only when hungry
- Measure your progress wisely
- Be persistent
- Avoid overeating fruit
- Avoid beer
- Avoid non-caloric sweeteners
- Review any medications
- Stress less, sleep more
- Eat less dairy products and nuts
- Supplement vitamins and minerals
- Use intermittent fasting
- Exercise wisely
- Achieve higher ketone levels
- Get your hormones checked
- Consider weight loss medications
For extra support on your weight loss journey, join our Connect community.
This guide is written for adults with health issues, including obesity, that could benefit from losing weight.
We don’t recommend counting calories, which is controversial. To learn more about the rationale for this, see our guide on restricting calories for weight loss.
Controversial topics related to a low-carb diet, and our take on them, include saturated fats, cholesterol, whole grains, red meat and whether the brain needs carbohydrates.
1. Choose a low-carb or high satiety diet

If you want to lose weight, consider starting by avoiding sugar and starch (like bread, pasta and potatoes). This is an old idea: for 150 years or more there have been a huge number of weight loss diets based on eating fewer carbs. What’s new is that reviews of modern scientific studies have repeatedly shown that low carb is at least as good, if not better, than other approaches to diet.4
Obviously, it’s still possible to lose weight on any diet – just eat fewer calories than you burn, right? The problem with this simplistic advice is that it ignores the elephant in the room: hunger. Most people don’t like to “just eat less,” as it may result in having to go hungry forever. Sooner or later, many will likely give up and eat without restriction, hence the prevalence of “yo-yo dieting.”5 While it should be possible to lose weight on any diet, some appear to make it easier and some to make it much harder.
The main advantage of the low-carb diet is that it may cause you to want to eat less.6 Even without counting calories, overweight people tend to eat fewer calories on low carb.7 Thus, calories count, but you don’t need to count them.
A 2012 study also showed that people who had lost weight experienced far less reduction in total energy expenditure (the number of calories burned within a 24-hour period) when they followed a low-carb diet compared to a low-fat diet during weight maintenance — a 300-calorie difference, in fact.8
According to one of the Harvard professors behind the study, this advantage “would equal the number of calories typically burned in an hour of moderate-intensity physical activity.” Imagine that: an entire bonus hour of exercise every day, without actually exercising.
Recently, an even larger and more carefully conducted study confirmed this metabolism-sparing effect, with different groups of people who had lost weight burning an average of between 200 and almost 500 extra calories per day on a low-carb maintenance diet compared to a high-carb or moderate-carb diet.9
But reducing carbs isn’t the only way to lose excess weight without hunger. Eating higher satiety foods may also help you accomplish your health and weight loss goals. Higher satiety foods tend to have higher protein percentages, lower energy density, higher fiber, and lower hedonic characteristics. You can read more about higher satiety eating in our evidence-based guide.
And the best part is that higher satiety eating works with almost any eating pattern — including keto and low carb eating.
Bottom line: A low-carb diet can reduce your hunger, making it easier to eat less. And it might even increase your fat burning at rest. Study after study shows that low carb works for weight loss and that on average it improves important health markers.10
In addition, higher satiety eating can help you lose excess weight with minimal hunger, and it is compatible with low carb and keto eating.
Why low carb can help you lose weight
How to lose weight with a low-carb diet
Learn more about keto and low-carb
Do you want to know more about exactly what to eat on low carb, how to do it, potential problems and solutions — and find lots of great recipes? Check out our keto for beginners guide. Alternatively, you can make low carb even simpler by signing up for our free two-week keto challenge.
2. Eat when hungry

Eating when hungry sounds simple: if you’re not hungry, you probably don’t need to eat yet.
When on a low-carb or keto diet you can trust your feelings of hunger and satiety again — something many people following a low-fat or standard American diet cannot do.11 Feel free to eat as many — or as few — times per day as you feel is right for you.
Some people eat three times a day and occasionally snack in between (note that frequent snacking could mean that you’d benefit from adding protein, fibrous veggies, or extra fat calories to your meals, to increase satiety). However, there’s some evidence that frequent snacking may not be wise when trying to lose weight.12 Some people only eat once or twice a day and never snack. Whatever works for you. Just eat when you’re hungry, and don’t eat when you aren’t.
It also helps that low-carb diets and higher protein diets — at least 20% of daily calories — tend to reduce hunger.
Studies demonstrate that people eating a very low-carb, ketogenic diet reduce their feelings of hunger and the amount of food they eat.13
Multiple other studies demonstrate that adding protein to your diet markedly reduces hunger and food intake.14
Our suggestion? Try a low-carb, higher protein approach and see what happens to your hunger levels.15
Read more about why eating when hungry is smarter than counting calories
3. Eat real, minimally processed food

Another common mistake when eating a low-carb diet is getting fooled by the creative marketing of special “low-carb” products.
Remember: an effective low-carb diet for weight loss should be based primarily on whole food.
Prioritize what humans have been eating for thousands or likely millions of years, e.g. meat, fish, vegetables, eggs, butter, olives, nuts etc.16
If you want to lose weight, avoid special “low-carb” products that are full of carbs. This should be obvious, but creative marketers are doing all they can to fool you (and get your money). They will tell you that you can eat cookies, pasta, ice cream, bread and plenty of chocolate on a low-carb diet, as long as you buy their brand. They’re often full of carbohydrates. Don’t be fooled.
How about low-carb bread? Be careful: if it’s baked with grains it’s certainly not low carb. But some companies still try to sell it to you as a low-carb option.
Low-carb chocolate is usually full of a kind of sugar alcohol — maltitol — that may actually be partially absorbed by the body, but which the manufacturer does not count as carbs. If the maltitol is absorbed, it is likely to raise blood sugar and insulin levels.17 The remaining carbs end up in the colon, potentially causing gas and diarrhea.
While low-carb chocolate made with erythritol or stevia is likely to be okay, you still have to consider that any sweeteners can maintain sugar cravings.18
Two simple rules to avoid being tricked into purchasing unhealthy “low carb” products:
- Don’t buy “low carb” versions of high carb stuff, like cookies, bars, chocolate, bread, pasta or ice cream – unless you are sure of the ingredients (ideally, by making it yourself).
- Avoid products with the words “net carbs” on them. That may be a way to deceive you.
Focus on eating good quality, minimally processed real food. Ideally, the food you buy shouldn’t even have a list of ingredients (or it should be very short).
A landmark 2019 study reported that the level of food processing was much more important than the macronutrient composition when it came to overeating.19 Those randomized to highly processed foods ate over 500 calories per day more than those eating less processed foods, despite an attempt to match the amount of protein, carbs, fat, and fiber.
Read more about fake low-carb products
Less moderation, more quality
Finally — you may want to forget about the old “everything in moderation” diet motto. It isn’t necessarily helpful advice for people who struggle with weight — in fact, it may be exactly the opposite.20
Don’t eat everything in moderation. Eat as much healthy food as you can, whenever you are hungry. Eat as little unhealthy food as you can – if possible, none at all.
4. Eat only when hungry

When eating low carb or higher satiety foods you should aim to eat when hungry (see tip #2 above). And if you’re not hungry? Don’t eat. Frequently eating more food than you need to stay satisfied will slow down weight loss.21 This, in fact, is so important that it’s worth a section of its own.
Limit unnecessary snacking
Unnecessary snacking can be a problem on a low-carb diet too. Some things are easy to eat just because they’re tasty and readily available. Here are three common traps to watch out for on a low-carb or keto diet:22
- Dairy products such as cream and cheeses. They work well in cooking, as they satisfy. But problems arise when you’re munching a lot of cheese in front of the TV in the evening — without being hungry. Be careful with that. Another problem might be having lots of cream with dessert, when you’re actually already full and just keep eating because it tastes good. Another common culprit is loads of heavy cream in the coffee, many times per day.
- Nuts. It’s very easy to eat until the nuts are gone, regardless of how full you are. A tip: According to science, salted nuts are harder to stop eating than unsalted nuts.23 Salted nuts tempt you to more overeating. Good to know. Another tip: Avoid bringing the entire bag to the couch – choose a small bowl instead.
- Low-carb baking. Even if you’re only using almond flour and sweeteners, snacking on baked goods and cookies usually represents additional eating when you’re not hungry — and yes, this will slow down weight loss.
Feel free to skip meals
Do you have to eat breakfast? Research has confirmed that the answer is no.24 Don’t eat if you’re not hungry. And this goes for any meal.
On strict low-carb or higher satiety diets the hunger and urge to eat tend to decrease significantly.25 If this happens, be happy! Don’t fight it by eating food you don’t want. Instead, wait for the hunger to return before you eat again. This will save you both time and money, while speeding up your weight loss.
Some people fear that they will lose control if they don’t eat every three hours. The concern that this “urge to binge” will blow their diets completely leads them to obsessively snack all the time.
This constant snacking may be necessary in order to control the hunger and craving that may arise during a diet high in sugar and starchy carbs, but it’s usually unnecessary on a low-carb diet. Hunger will only slowly return and you should have plenty of time to prepare food or grab a snack.
Bottom line: To lose weight in a sustainable way, eat when you’re hungry – but only when you’re hungry. Forget the clock and listen to your body instead.
Learn more



Tracking successful weight loss is sometimes trickier than you’d think. Focusing primarily on weight and stepping on the scale every day might be misleading, cause unnecessary anxiety, and undermine your motivation for no good reason. The scale is not necessarily your friend. You may want to lose fat – but the scale measures muscles, bone and internal organs as well. Gaining muscle is a good thing. Thus weight or BMI are imperfect ways to measure your progress. This is especially true if you’re just coming off a long period of semi-starvation (which may accompany calorie-counting), as your body may want to restore lost muscle. Starting weight training and gaining muscle can also hide your fat loss. Losing fat and gaining muscle means great progress, but you may miss this if you only measure your weight. Thus it’s best to quantify body composition as you lose weight. You can do this with a DEXA scan, hydrostatic weights, plethysmography scales and others. But if these are not available, it is smart to also track the disappearance of your belly fat, by measuring your waist circumference. I recommend aiming for “good” but it’s not always realistic. Young people can usually achieve this, but for some middle-aged or older people, it may be a major victory to get all the way to “decent”.26
But even your waist size may be misleading. A 37 inch waist for someone 6 feet 7 inches isn’t the same as for someone who is 5 feet 2 inches. Therefore, your waist to height ratio may be an even better measurement. Simply divide your waist (in inches or centimeters) by your height. A value below 0.5 suggests a lower risk for insulin resistance and metabolic dysfunction.27 You can learn more in the diagnosis section of our insulin resistance guide. I suggest measuring your waist circumference and weight before starting your weight loss journey and then perhaps once a week or once a month. Write the results down so that you can track your progress. If you want, you can measure more areas: around the buttocks, the chest, the arms, legs, etc. Please note that your weight can fluctuate up and down several pounds from day to day, depending on fluid balance and digestive system contents. Don’t worry about short-term changes, follow the long-term trend instead. These markers are frequently improved on a low-carb diet, even before major weight loss.28 Re-checking these health markers after a few months can be great for your motivation as they’ll usually show that you’re not just losing weight, you’re gaining health too. PS: Don’t have a measuring tape at home? Try these options: It usually takes years or decades to gain a lot of weight. Trying to lose it all as quickly as possible by starving yourself does not necessarily work well in the long term; instead it may be a recipe for “yo-yo dieting”.29
In addition, you need to set realistic expectations for health and weight loss goals. You can read more in our detailed guide on realistic expectations. It’s common to lose 2-6 pounds (1-3 kg) within the first week on a strict low-carb or high satiety diet, and then on average about one pound (0.5 kg) per week as long as you have a lot of weight remaining to lose.30 This translates into about 50 pounds (23 kilos) per year. However, weight loss doesn’t occur at this rate in everyone. Young males sometimes lose weight faster than this.31 Post-menopausal women may lose at a slower pace.32 People on a very strict low-carb diet may lose weight quicker, as well as those who exercise a lot (a bonus).33 And the more weight you vae to lose, the faster you can start to lose it— although initially, some of the weight you lose will be due to water loss. As you get closer to your ideal weight, the loss may slow down until you stabilize at a weight that your body feels is right. Very few people become underweight on a low-carb or higher satiety diet as long as they eat when hungry. Are you coming off a period of semi-starvation (which can occur with calorie-counting)? Focus on your waist circumference and health markers (see tip #4) at first, as it sometimes takes several weeks before weight loss is apparent.34
Expect weight loss plateaus: months where nothing seems to happen on the scale. Everybody hits them.35 Stay calm. Keep doing what you’re doing and eventually things should start happening again (if not, check out the other 17 tips). More: Top 10 tips top break a weight loss stall Losing a lot of weight long term and keeping it off will likely not happen unless you change your habits forever. If you lose weight and then return to living exactly the way you did when you gained weight, don’t be surprised when the excess weight returns. It normally will. But that doesn’t mean that the diet you used to initially lose excess weight is the only diet that will work for you. Clinical experience suggests that someone may do great at first with a ketogenic diet, but then may continue long-term success with a moderate carb higher satiety diet. The key is to keep an open mind and be willing to adjust along the way. Maintaining weight loss usually requires long-term change and patience. As tempting as it may be, don’t fall for one of these magical diet scams. Forget quick fixes: If you lose some weight every month, eventually you may get rid of all your excess weight. That’s inevitable progress. That’s what you want. PS: Long-term change is hardest in the beginning, especially during the first couple of weeks. It’s like quitting smoking. Once you develop new habits it becomes easier and easier every week. Eventually it may come naturally. For inspiration and tips, check out some of our long-term weight maintenance success stories: Keep reading!
5. Measure your progress wisely

Here’s how to do it:
Compare your result to these recommendations:
Measuring progress
If you can, check other important health markers when starting out, like these:
6. Be persistent

What to aim for
Initial stalls
Weight loss plateaus
How to keep the weight off long term
How to lose weight faster
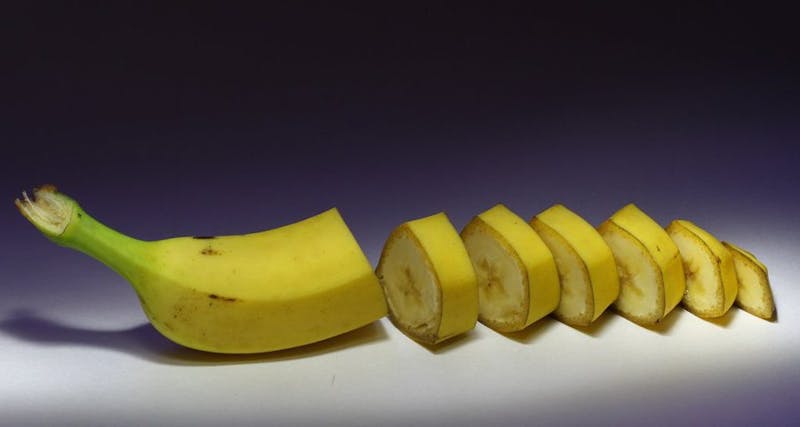
This piece of advice is controversial, as fruit has an almost magical health aura today. While fruit does contain fiber, antioxidants, and important vitamins, it also contains a fair amount of sugar – around 10% by weight (the rest is mostly water).36 Just taste an orange or a grape. Sweet, right? Eating whole fruits in moderation – especially ones that are low in sugar, like berries – can absolutely be part of a healthy diet. The soluble fiber in fruit can help with short-term satiety; it also reacts with water in your gut to form a thick gel that helps delay and reduce the amount of sugar absorbed from that fruit. In fact, up to 30% of the sugar from fruit may not be absorbed. 37
Larger quantities of fruit, however, will deliver a significant sugar load to your intestines. Even if only 70% of that sugar is absorbed, 70% of a big number is still a big number. For example, five servings of fruit per day can be equivalent to the amount of sugar in 16 ounces (500 ml) of soda – 52 grams of sugar!38
Most people believe that fruit is natural, but today’s fruits in the grocery store have very little in common with what fruits looked like before they were cultured. Modern domesticated fruits are larger, less bitter, and have thinner peels and smaller seeds. This makes them tastier and easier to eat – and because of their increased size, they may provide more sugar per piece of fruit than their earlier counterparts. Beer contains rapidly digested carbs that shut down fat burning. That may be why beer is sometimes referred to as “liquid bread.” There’s a good reason for the term “beer belly.”39
Here are smarter (lower-carb) alcoholic options when trying to lose weight: These drinks hardly contain any sugar or digestible carbohydrates so they’re better than beer. However, large amounts of alcohol might slow weight loss, so moderation is still a good idea. 40
7. Avoid overeating fruit
Isn’t fruit natural?

8. Avoid drinking beer
 Low-carb fruits and berries – the best and the worst
Low-carb fruits and berries – the best and the worst 
According to scientific studies, non-caloric sweeteners may increase appetite and maintain cravings for sweet food.42 And one recent independent study showed that switching drinks with non-caloric sweeteners to water helped women lose weight.43
Study: Avoiding diet beverages helps women lose weight This may be related to the increased insulin secretion seen with some non-caloric sweeteners.44 Maybe that is why something odd happened when Dr. Eenfeldt tested Pepsi Max. If you’re having trouble losing weight, we suggest that you avoid sweeteners. As a bonus, you’ll likely find it easier to enjoy the natural sweetness of real food, once you’re no longer adapted to the overpowering sweetness of processed low-carb food products and “diet” sodas. Do you find the idea of avoiding sweeteners almost impossible to imagine? Addiction-like relationships to sugar and carbohydrate-rich foods can be overcome. Check out this video with addiction specialist Bitten Jonsson, RN Many prescription drugs can stall your weight loss. Discuss any change in treatment with your doctor. Here are the three most common offenders: A. Eat fewer carbs, which makes it easier to lose weight. The fewer carbs you eat the less insulin you need.46 Remember to work closely with your healthcare provider to ensure you safely lower your doses. B. If this isn’t enough, treatment with metformin (an insulin sensitizing drug) can decrease the need for insulin (at least for people with type 2 diabetes).47
C. If this is not enough to get off insulin (again, for people with type 2 diabetes), discuss with your doctor if it is appropriate to try a drug in one of the newer classes like the GLP-1 analogues or DPP-4 inhibitors. There are many different options within these two categories; what you need to know is the drugs in these classes reduce the need for insulin and may also cause weight loss by other mechanisms — beyond just the effect of using less insulin. You can learn more in our guide on starting low-carb or keto with diabetes medications.
These other medications can also cause problems:
9. Avoid non-caloric sweeteners

Many people replace sugar with non-caloric sweeteners in the belief that this will reduce their calorie intake and cause weight loss. It sounds plausible. Several studies, however, have failed to show obvious positive effect on weight loss by consuming non-caloric sweeteners instead of plain sugar.41
Sugar addiction
10. Review any medications
 Other diabetes medications, like drugs that stimulate the secretion of insulin by the pancreas (e.g. sulfonylureas), often lead to weight gain.48 These include: Amaryl (glimepiride), Glucotrol/Minodiab (glipizide), Euglucon (glibenclamide), and Daonil (glyburide). Additional diabetes medications like Actos (pioglitazone), Starlix (nateglinide) and Prandin/NovoNorm (repaglinide) also encourage weight gain. But not metformin. More on diabetes
Other diabetes medications, like drugs that stimulate the secretion of insulin by the pancreas (e.g. sulfonylureas), often lead to weight gain.48 These include: Amaryl (glimepiride), Glucotrol/Minodiab (glipizide), Euglucon (glibenclamide), and Daonil (glyburide). Additional diabetes medications like Actos (pioglitazone), Starlix (nateglinide) and Prandin/NovoNorm (repaglinide) also encourage weight gain. But not metformin. More on diabetes
 Full low-carb sweeteners guide
Full low-carb sweeteners guide Have you ever wished for more hours of sleep and a less stressful life in general? Most people have – stress and lack of sleep can be bad news for weight. Chronic stress and inadequate sleep may increase levels of stress hormones such as cortisol in your body. This can cause increased hunger, resulting in overeating and weight gain.54 If you’re looking to lose weight, you should review possible ways to decrease or better handle excessive stress in your life. Although this often demands substantial changes, it may immediately affect your stress hormone levels and perhaps your weight. You should also make an effort to get enough good sleep, preferably every night. Strive to wake up refreshed of your own accord, independently of the alarm clock. If you’re the kind of person who always gets brutally woken up by the alarm ringing, you might never be giving your body completely adequate rest. One way to combat this is to go to bed early enough for your body to wake up autonomously before the alarm clock goes off. Letting yourself get a good night’s sleep is another way of reducing stress hormone levels. Sleep deprivation, on the other hand, goes hand in hand with sugar cravings.55 It also has an adverse effect on self-discipline and makes it painfully easy to give in to temptation (it’s no coincidence that induced sleep deprivation is a common interrogation technique). Similarly, sleep deprivation weakens your resolve to work out. Do you have trouble sleeping even if there’s ample time for it? Here are five helpful tips56: Finally, make sure that your bedroom is dark enough, and stays at a pleasant temperature. Sleep well! Many may find the above guidelines difficult to follow, perhaps because of a lack of time (or the equivalent – small children!). But stressing less and sleeping more doesn’t just feel good. It can also play a part in helping you get leaner.
11. Stress less, sleep more

Sleep issues?
Difficult, but worthwhile
Can you eat as much as you like and still lose weight? This often works well with a low-carbohydrate or higher satiety diet, as appetite regulation often improves.57
However, despite the fact that a low-carbohydrate diet generally makes it easier to eat just enough, there are foods classified as low carb which are lower satiety foods and may become a problem in larger quantities. If you find yourself having a hard time losing weight on a low-carb diet, you could try shifting to a higher satiety diet and reducing: High fat dairy products contain varying amounts of lactose (milk sugar) and lots of calories from fat — both of which could slow down weight loss when over-consumed. Consequently, cutting back on high fat dairy products may help accelerate weight loss. Remember that, gram for gram, fat has twice the calories of carbs or protein; therefore, high-fat, highly palatable foods can deliver a huge calorie load before you know it.58
When it comes to butter, you don’t need to worry about extra carbs, as butter is almost pure fat. But, like any other source of fat, if butter is over-consumed, the calories can add up and your dietary fat will likely be burned for fuel instead of body fat. Low-carb and dairy-free recipes Nuts, the second food to watch, contain a fair amount of carbohydrate in addition to a significant amount of calories from fat, and it’s very easy to unwittingly scarf down large quantities.59 That’s why nuts are a low satiety per calorie food. The high calorie load delivered by handfuls of nuts can thwart weight loss. If you are trying to follow a strict ketogenic diet, with a 20 grams of carbs per day allowance, you should also note that cashew nuts are among the worst carb-wise – you’ll find that they contain around 20% carbohydrate by weight. This means that consuming 100 grams of cashews (which happens in a flash!) will fill your daily quota. Peanuts tend to be around 10-15% carbohydrate – not putting them in the clear either. So, for those of you having trouble losing weight: use nuts sparingly. And for those of you on a strict keto diet, know that the most harmless ones carb-wise are macadamia nuts (usually around 5% carbs), or Brazil nuts (4%).
12. Eat less dairy products and nuts

 Low-carb nuts – the best and the worst
Low-carb nuts – the best and the worst Your body needs a certain amount of essential vitamins and minerals to function properly. What happens when you don’t get enough of them? What happens when you eat too little food or when the food you eat isn’t sufficiently nutritious? It is possible that our bodies catch on and reply by increasing hunger levels. After all, if we eat more, we increase the chances of consuming enough of whatever nutrient we are lacking. On the other hand, reliable access to vitamins and minerals could perhaps mean decreased hunger levels and decreased cravings, thereby promoting weight loss. The above is speculation without strong supporting evidence. But there are a few studies which suggest it might not be far from the truth. A lack of vitamin D could be the most common deficiency in northern countries such as Canada and some of the US. Overall, the research on the relationship between vitamin D and weight is conflicting, and it cannot be concluded that taking vitamin D will cause weight loss.60 Nonetheless, there are studies indicating that, when compared to a placebo, a vitamin D supplement could help decrease your fat mass or waist measurement, even in the absence of weight loss.61
In one of the studies, 77 overweight or obese women received either a supplement of 1000 units of vitamin D or a placebo, every day for 3 months. Although the total weight loss was similar, those who took the vitamin D supplement decreased their body fat by 2.7 kg (6 pounds), on average. This was significantly more than the placebo group, whose average fat loss was only 0.4 kg (less than 1 pound).62 The data regarding vitamin and mineral supplementation for weight loss is sparse and of very low quality overall. However, there is a clinical trial from 2010 involving around a hundred women with weight issues, separating them into three groups. One group received a daily multivitamin supplement, the other a daily calcium supplement, and the last group only a placebo. The study went on for six months. Unsurprisingly, the results showed that nothing had happened to the weight of the women receiving calcium or the placebo. However, the group that took the multivitamin lost more weight – an average of 3.6 kg (8 pounds) more – and improved several health markers. Among other things, their basal metabolic rate (the rate at which the body burns calories when at rest) increased.63 Although the differences were small, they were statistically significant. Nutrient-dense, whole food is certainly the foundation of weight loss. But an adequate amount of vitamin D can be difficult to ingest via food, especially for those who are vegetarian or don’t eat fatty fish (the main dietary source of vitamin D) on a regular basis. In the case of a lack of sun (such as during the darker months of fall and winter), it may be wise to supplement for other health reasons – and perhaps for your body composition. In addition, if you’re overweight and not entirely sure that your diet provides enough nutrients, it may be worthwhile to take a multivitamin pill. While the evidence is weak that either of these interventions will help with weight loss, there is likely little downside and you may see a small benefit.
13. Supplement vitamins and minerals

Vitamin D
Multivitamins
Conclusion
14. Use intermittent fasting

There are many things to consider before moving on to tip #14, but don’t let this deter you. Intermittent fasting can be a powerful tool when trying to lose weight. It may be perfect if you are stuck at a weight loss plateau despite “doing everything right” – or to speed up your weight loss.64
Intermittent fasting means exactly what it sounds like: not eating during a specified time interval.
Recommended first option – 16:8
Probably the most popular option is fasting for 16 hours (including sleep), which is usually easy to do on a low-carb or high satiety diet. It requires trading breakfast for a cup of coffee (or some other non-caloric fluid) and having lunch as the first meal of the day. Fasting from 8 pm to 12 noon – for example – equals 16 hours of fasting. Another option is to skip dinner: eat breakfast and lunch within 8 hours — for instance, 8 am to 2 pm — and then don’t eat again until 8 am the next morning.
There are many other versions of intermittent fasting, but this 16:8 method (16 hours of not eating with an 8-hour eating window) is the one we recommend as a first option. It’s often effective, generally easy to do and does not require counting calories.
You can do a 16:8 fast as often as you like. For example twice a week, on weekdays only, or every single day. In fact, on a low-carb or keto diet, some people spontaneously fall into this habit, as their appetite is reduced (see weight loss tip #4, eat only when hungry).
Although it’s possible that doing it more frequently may improve your results, long-term studies are lacking.65 Therefore, we simply don’t know if frequent fasting will decrease resting metabolic rate in a similar manner to continuous caloric restriction, making weight loss and maintenance more difficult in the long run.
Also, clinical experience suggests that some people feel the urge to overeat calories during their eating window when they first try intermittent fasting. If this is the case, it may not be the right time to try IF. Instead, you may benefit from focusing on higher satiety eating first, so that you have less hunger and feel less of an urge to overeat during your eating window.
Other kinds of intermittent fasting
There are many other options. Basically, the longer periods may be harder to do, but they can certainly be effective. Here are two more common options:
- Fasting for 24 hours (often dinner to dinner) once or twice a week. This can be effective and easy to do for some people, especially on a keto diet, which usually reduces appetite. You can learn more about eating one meal a day (OMAD) in our evidence-based guide.
- The 5:2 diet. Eat as much as you need to feel satisfied 5 days of the week and then eat calorie-restricted on two days (500 calories per day for women, 600 calories for men). This requires calorie counting and more planning, but some people still find they enjoy it.
What about eating when hungry?
Doesn’t advice on intermittent fasting contradict the advice to eat when hungry? Yes it does, somewhat.
We recommend eating when hungry as a first option, and we recommend always eating until you feel satisfied at meals. But if this is not effective enough, then intermittent fasting can be a useful tool in your tool kit. Remember – and this is crucial – that between fasting periods you’re still supposed to eat until satisfied.
Intermittent fasting is not the same thing as obsessively counting calories and starving yourself 24-7. Starving yourself may be a recipe for misery and failure.
Intermittent fasting is about eating all that your body needs, while still allowing it to sometimes briefly rest from constant feeding.
What’s acceptable to drink during fasts?
During a fast you can’t eat, but you should definitely drink. Water is the drink of choice, but coffee and tea are also great options. During longer fasts it can be wise to add some salt too, or drink bouillon.66
Anything you drink should ideally be zero calories. But it may be acceptable to modify this by adding a small amount of milk or cream in your coffee or tea – if you absolutely need it to enjoy your drink.
What to eat between fasts
So what should you eat when you are not fasting? Well, if your goal is to lose weight, we suggest following all the tips above, including eating a low-carb or higher satiety diet. Pairing either of these with intermittent fasting is a great combination.
On a low-carb diet, hunger is typically reduced, making it much easier to fast. Also, glycogen stores in the liver should be lower while eating low carb, meaning that fasting may flip the metabolic switch to fat burning mode earlier than if not on a carb-restricted diet. This may be one of the mechanisms that enhances weight loss.67
So, while on a low-carb diet the fasting periods may become both easier to do and more effective. 1 + 1 equals 3.
Who should not do intermittent fasting
Intermittent fasting can be a great idea, but not everyone should do it:
- If you have a history of disordered eating then intermittent fasting may not be right for you. We recommend consulting with your physician before trying intermittent fasting.
- If you are stressed out or sleep deprived, then take care of that problem first (see weight loss tip #11) or fasting may be too stressful for your body.
- If you are on any medication – especially insulin – the doses may need to be adjusted when fasting. Discuss this with your doctor first.
- Growing children, pregnant women and breastfeeding women should not do longer fasting periods, as they have increased nutrient needs. We recommend eating when hungry and using the other tips in this guide if weight loss is needed.
More
Do you wonder why this weight loss tip doesn’t show up until number 15 on the list? It’s because exercise is greatly overrated as a single intervention for weight loss.68
Have you ever watched “The Biggest Loser”? The participants take leave from their jobs (and family) for months. They are allowed only small portions of food, and work out as though it were their full-time job – 40 hours a week, sometimes more. This method is clearly unsustainable for the average person in the long run.69
Just taking the stairs instead of the elevator, or getting off the bus one stop earlier, is probably not going to change the numbers on your bathroom scale. It’s a myth. Studies show that if you just start exercising, you’re likely going to need at least 30-60 minutes of workouts per day to noticeably lose weight.70 Part of the reason is that exercise makes people hungrier, and eating more reduces its beneficial effect on weight.71
While the effect of exercise on our weight is overrated, exercise can still provide meaningful health improvements, even without weight loss. You can learn more in our guide on exercise. But it’s not a good idea to eat unhealthy processed food and drink sugar water (so-called “sports drinks”), and then exercise for hours daily just to compensate. Metaphorically that’s like digging a hole, into which you put your ladder, on which you stand and paint the basement-level windows of your house. Exercise cannot compensate for other behaviors or issues in your life. Those must be addressed first. If, on the other hand, you’ve already taken care of steps 1-14, you should have a rested and recharged body which is already happily burning fat. In this case, increased activity can accelerate your weight loss, fat mass loss and reduction of insulin levels.72 Also, don’t forget that the non-weight-related health effects of exercise are quite impressive. For even more impressive effects on body composition, aim for exercise forms which elicit a positive hormonal response. This means lifting heavy things (strength training), or interval training. Such exercise increases levels of the hormone testosterone (primarily in men) as well as growth hormone.73 Not only do greater levels of these hormones increase your muscle mass, but they also decrease your visceral fat (belly fat) in the long term. As a final bonus, exercise can both make you feel and look better. What kind of activity fits you?
15. Exercise wisely

The good news
Hormonal effects
We’ve now arrived at tip number 16. If you’re still having trouble losing weight, despite following the 15 pieces of advice listed above, it might be a good idea to bring out a controversial option: higher ketone levels (this advice applies only to people following a ketogenic diet). Why is it controversial? For most people, “low” or “higher” ketone levels don’t make a difference for health and weight loss, and in general we do not recommend shooting for a specific ketone level.74 However, for some people stalling at weight plateaus while on a low carb diet, trying to raise ketone levels may be of benefit. So how does this work? A quick run-through: The first tip was to eat low carb. This is because a low-carb diet lowers your levels of the fat-storing hormone insulin, allowing your fat deposits to release their stored energy and shrink.75 This tends to cause you to want to consume fewer calories than you expend – without hunger – and lose weight.76 Several of the tips mentioned earlier are about fine-tuning your diet to better this effect. Ketosis is a state in which the body is efficiently burning fat. Even the brain runs on fat, in the form of ketone bodies. These are energy molecules in the blood (like blood sugar) which become fuel for our brains after being converted from fat by the liver.77
To encourage ketone production, the amount of insulin in your bloodstream must be low. The lower your insulin, the higher your ketone production. And when you have a well-controlled, sufficiently large amount of ketones in your blood, it’s basically proof that your insulin is very low – and therefore, that you’re enjoying the maximum effect of your low-carbohydrate diet.78
Today, there are reasonably-priced gadgets available for measuring ketone levels at home. One needle prick of the finger, and in just a few seconds you’ll know your blood ketone level. Here are a few pointers on how to interpret blood ketone results: Ketone levels can also be measured in a more old-fashioned way, with urine test sticks (sold prescription-free in pharmacies or on Amazon81). Ketone sticks give less reliable results for several reasons, and the above recommendations can’t be straightforwardly applied to them. They are, however, much cheaper. Breath meters provide another method for measuring ketone levels. Some breath meters give a range of ketosis — mild, moderate, or high — while others give a quantitative result. The up-front cost to breath meters is usually higher than blood meters, but the long-term cost may be lower for those who test frequently, as there are no recurring expenses as there are with blood ketone testing strips. Which method is best? That depends on your goals and how often you want to test. Diet Doctor’s own Jenni Callihan tested numerous products and her guide describes the benefits and drawbacks to each device. Many who firmly believe they are eating a strict low-carb diet are surprised when they measure their blood ketones. They may be at around only 0.2 or 0.4. Why? First, you should make sure you are avoiding all obvious sources of carbohydrate (sweets, bread, spaghetti, rice, potatoes). Next, check for “hidden carbs” in salad dressings, dips, and from other sources like alcohol. In an effort to improve fat-burning, thereby increasing ketone levels, you may consider adding intermittent fasting or exercise to your routine (see tips #14 and #15 above). Finally, make sure you are eating adequate amounts of protein. A keto diet for weight loss should be at least a moderate protein diet. We recommend 1.2 to 2.0 grams per kg of reference body weight per day.82 Check out our target protein ranges to find out how much protein you should be aiming for each day. Having higher ketone levels most of the day for a prolonged period of time (say, a month) will ensure that you experience the maximal hormonal effect from eating a low-carb diet.83 If this doesn’t result in noticeable weight loss, you can be fairly certain that too many carbs are not part of your weight issue and are not the obstacle to your weight loss. There are, in fact, other causes of obesity and being overweight. The next two tips in this series might help you. Order a ketone meter online and start measuring. There are a few different models.84 Unfortunately these meters can be quite expensive to use, depending on how often you test. Fortunately, with more competition, the price of test strips has come down to about $1 per strip. Here’s a complete package85 with everything you need to check your blood ketone levels. Learn much more about ketogenic diets and ketosis: A quick guide to ketogenic diets Watch my video interview with the American doctor Peter Attia, on a strictly ketogenic low-carb diet: Very Low Carb Performance If you have type 1 diabetes, you should not purposefully try to increase your ketone levels – it may be risky. If you have ketones in your blood at all, you must be sure that your blood sugar levels are normal and you are getting adequate insulin. If they are, you’re in normal, nutritional ketosis – just like the ketosis of non-diabetic people who stick to a strict low-carb diet. High blood sugar levels coupled with high blood ketones, on the other hand, will mean that you have a pathologically low level of insulin – something those without diabetes don’t experience. This can lead to ketoacidosis – a potentially life-threatening condition. If this happens, you’ll need to contact your healthcare provider immediately or have someone take you to the hospital to be checked out. Coveting really high blood ketones for weight control is not worth the risk for people with type 1 diabetes.
16. Achieve higher ketone levels

Warning: Not recommended for people with type 1 diabetes, see below.Ketosis
Measuring ketones
Ketones in urine
Breath ketone meters
How to achieve higher ketone levels
If it doesn’t work
Try it
More
A word of warning
So you’ve followed the previous tips, implemented major lifestyle changes, and established that neither medication nor vitamin deficiency is an issue. You’ve even tried increasing your ketone levels for a while (ensuring low insulin levels). And you still can’t hit the normal weight mark? If this applies to you, it may be time to consider the possibility that hormonal imbalances are the cause of your troubles. There are three common problem areas: Some people, most often women, can suffer decreased metabolism as a result of thyroid hormone deficiency. Common symptoms of hypothyroidism are: In these cases, weight gain resulting from decreased metabolism usually does not exceed 15 pounds.86
Your doctor can easily arrange for you to take a blood test to measure the concentration of thyroid stimulating hormone (TSH). If the test comes back and everything looks good, your thyroid gland is probably fine. However, it is possible to have mild hypothyroidism, even though the TSH is within the normal range. If your TSH is in the upper portion of the normal range, yet you suspect you may have hypothyroidism, it is worth measuring a free T4 (thyroid hormone level) and thyroperoxidase (TPO) antibodies. If the free T4 is frankly low or the TPO antibody test returns high, it is possible – but not definite – that you will benefit from thyroid hormone treatment.87
Is it possible to avoid becoming deficient in thyroid hormone? Maybe. Although there aren’t any interventions known to stop an autoimmune attack on the thyroid, normal thyroid function requires adequate vitamins and minerals, including iodine, selenium, and iron.88
What if you have optimized your vitamin and mineral intake, but you still suffer from low levels of thyroid hormone? The most common cause of hypothyroidism is an autoimmune reaction against the thyroid gland. This is typically treated with supplemental T4 in the form of levothyroxine, which the body converts into the active form of thyroid hormone, called T3. Some people with hypothyroidism will also benefit from the addition of T3 (liothyronine) to their T4 therapy. Still other people will prefer desiccated pig thyroid (contains T4 and T3), though this treatment remains controversial and is not embraced by all healthcare providers.89 Regardless of what form of thyroid hormone replacement you choose, the key is making sure you follow your levels and symptoms to make sure you aren’t over- or under-replacing thyroid hormones. Sex hormones also affect your weight: Women: Women can suffer from the endocrine disorder PCOS – polycystic ovarian syndrome – which elevates testosterone and insulin levels. This can mean weight gain and menstrual disorders (very common), infertility, acne, and male pattern hair growth (such as facial hair). A low-carbohydrate diet may help treat this condition.90 More on PCOS. During menopause, estrogen levels can fluctuate widely, eventually dropping to low levels as the ovaries lose their ability to make it. This time of life is often associated with a drop in metabolic rate and some weight gain, especially around the gut (so-called central obesity). Current evidence suggests that hormone replacement therapy with estrogen may help achieve a more favorable body composition, though its effect on weight is minimal at best.91
Learn more: Top 10 tips to lose weight on low carb for women 40+ Top 8 tips to lose weight during menopause Men: From middle-age onward, testosterone levels gradually decline, which is considered normal. Sometimes, the decline is larger than what would be considered normal. This can be associated with some weight gain, typically around the gut, as well as decreased muscle mass.92
Mild testosterone deficiency may be partially addressed by engaging in smart exercise routines and supplementing vitamin D.93
A more significant deficiency, confirmed by blood testing, is typically treated with testosterone replacement therapy. Both men and women should take into account, however, that supplementation of testosterone or estrogen for years on end can come with potential side effects.94
It may be wise to accept that you don’t (and shouldn’t!) have the body of a 20-year-old when you’re at least twice that age. A better option might be to focus on a healthy lifestyle instead, and be as happy and grateful as you can for the body you have. Another possible hormonal issue behind stubborn weight issues may be the main stress hormone, cortisol. Too much cortisol can increase hunger, bringing subsequent weight gain, especially around the midsection.95
The most common causes of elevated cortisol are chronic stress and lack of sleep (see tip #11), or cortisone medication (tip #10). It is very important to realize that it’s the underlying stress and sleep that need to be addressed; supplements that promise to lower cortisol levels will likely not help you lose weight if you haven’t corrected the underlying cause.96
In extremely rare cases, you could be dealing with a specific kind of tumor that drives cortisol production. The condition is called Cushing’s syndrome. If you suspect you’re suffering from this, consult your doctor, who will run appropriate tests or refer you to an Endocrinologist. It sounds like a dream. Keep living like you already do, take a daily pill, and effortlessly lose your excess weight. This is why weight loss medicines are a billion dollar industry. So do they work? Yes, somewhat. But the majority are not as effective as you might think and they may come with significant side effects. Most available drugs result in modest weight loss (about 5% of body weight on average), sometimes at the expense of bothersome side effects. More recent medications offer greater weight loss, up to 10 or even 15% of body weight, but in order to maintain any weight loss benefit you receive, you must continue the drug indefinitely.97 That’s right – if you stop the drug, you will likely regain the weight you lost, plus extra if your weight was already on an upward trajectory before starting the drug. The internet is full of claims of magic supplements that can make you thin. Unfortunately, the only thing they’ll make thin is your wallet. This is true even if they were once mentioned on Dr. Oz – you know that’s an entertainment show, right? Any prescription-free supplements for sale that are not dangerous or illegal are likely to have a small or negligible effect on your weight. This is true even for the vitamin supplements mentioned in advice #13 – the effect is definitely small, but in that case it’s also safe – maybe even healthy – and also dirt cheap, making it a potentially smart bonus (note that we sell no supplements whatsoever and make no money from this piece of advice). There are also prescription free “carb blockers” out there, that are supposed to stop the body from absorbing carbs we eat. The effects tend to be relatively tiny though, even in studies funded by the companies selling the products.98 It’s definitely more effective to not eat the carbs in the first place (it’s also free). In the US, phentermine is relatively inexpensive, generally well-tolerated, and modestly effective for many people. Because it is only FDA-approved for short-term use, many doctors specializing in weight management will continue to prescribe it “off-label” as a long-term strategy, if the person is doing well on the drug, as long as that person is willing to accept the risks. To date, there have not been any studies documenting negative consequences of this strategy. Nonetheless, these drugs have the potential side effects of insomnia, heart palpitations, headache, and elevated blood pressure.99
It is therefore important to be monitored closely, at least in the first few months of treatment, to make sure that blood pressure and heart rate aren’t rising too much. Also note that these drugs are controlled substances, requiring a special prescription. Let’s move on to another older drug, Xenical (orlistat), also for sale prescription-free in a lower dose as Alli. This drug prevents the body from digesting fat in the intestines. Instead it just passes through you and ends up in the toilet — or (worst case) in your pants. Side effects – mostly seen if consuming a meal with a significant amount of dietary fat – include stomach cramping, gas, leaking oily stool, and being unable to control bowel movements. Because the negative reinforcement of these side effects encourages the user to avoid dietary fat, this medication is generally incompatible with a low-carb diet, which tends to be higher in fat. However, if your version of low carb tends to be very high in protein and low in fat, this pill might give you that extra boost you need; otherwise, you may want to forget about orlistat. Many doctors already have. Qsymia combines a small dose of phentermine (see “Older appetite suppressants,” above) with a small dose of topiramate, an old anti-seizure drug. This is available in the US, but it got rejected in Europe (where the risks were judged worse than the benefits). Qsymia, like most other weight loss pills, can be modestly effective if pricey. But the side effects are sometimes intolerable: drowsiness, fatigue, depression, attention disturbance, memory impairment, and impaired psychomotor skills (i.e. becoming clumsy). Contrave (US) or Mysimba (EU) is a combination of bupropion (an old antidepressant) and naltrexone (an old opioid receptor blocker). This is another modestly effective, pricey drug that works on brain receptors to control appetite. Side effects include: nausea, constipation, headache, risk of suicidal thoughts and seizures. And then there is the reigning champion of weight loss drugs — GLP1 agonists including Saxenda (liraglutide) and Ozempic or Wegovy (semaglutide). Fortunately this one actually shows some promise and can speed up weight loss significantly. This drug is an injected variant of a satiety hormone called GLP-1. It slows down how quickly the stomach empties and tells the brain that you don’t need to eat yet – not a bad idea for losing weight. Liraglutide was initially used to control blood sugar in type 2 diabetes – under the brand name Victoza – where it has the nice side effect of significant weight loss.100
Testing on people with obesity (without diabetes) shows that at higher doses the drug is fairly effective as a pure weight loss treatment, with patients losing on average 12.3 pounds (5.6 kilos) more than a placebo group after one year.101
Unfortunately, Saxenda can cost upwards of $1000 per month. In both the US and Europe, Victoza (the same drug at half the dose) may be significantly less expensive. At this lower dose, the resulting weight loss is about 75% of the weight loss seen with Saxenda. Victoza is currently approved only for treating type 2 diabetes.102
The main side effect of Saxenda/Victoza is what happens if the satiety effect becomes too strong: nausea and vomiting. This is quite common when starting out, so it’s necessary to start with a low dose and then slowly increase it as the body adapts to the medication. Semaglutide, another GLP-1 analogue (similar to liraglutide), has been used to control blood sugar in type 2 diabetes since 2017. It has also been found to promote substantial weight loss – likely better than any drug currently available – in a trial of overweight people without diabetes.103 TThe FDA approved semaglutide for use with weight loss, and many feel this it is a “gamechanger” when it comes to medical weight loss. If you have type 2 diabetes, there is another class of diabetes drug that can result in noticeable weight loss: the SGLT 2 inhibitors. Examples include: Farxiga (dapagliflozin), Invokana (canagliflozin), Jardiance (empagliflozin), and Steglatro (ertugliflozin). Unfortunately, these drugs carry an increased risk of ketoacidosis in both type 1 and type 2 diabetes; this risk may be accentuated by a strict low-carb or keto diet. Therefore, it’s not recommended to take a medication in this class while on a strict low-carb diet.104
There is no weight loss drug that easily makes people thin. These medications all have potential side effects and most are not very effective. While GLP-1 analogues like liraglutide and semaglutide show promise, they are incredibly expensive and, like all weight loss drugs, they only work for as long as you take them. Many people who want to lose weight have more than 5-10% to lose. That’s why even the best weight loss drug can only be an optional complement to dietary and lifestyle interventions. That’s why this piece of advice is number 18 out of 18. It may be a helpful addition for some people, but the advice higher on the list is what can make the biggest difference.
17. Get your hormones checked

Thyroid hormone
Sex hormones
Stress hormones
18. Consider weight loss pills

Prescription-free supplements

Older appetite suppressants
 In the US, it’s still possible to get amphetamine-like appetite suppressants that are FDA-approved for less than 12 weeks of continuous use. These drugs are not approved in the EU. Examples include:
In the US, it’s still possible to get amphetamine-like appetite suppressants that are FDA-approved for less than 12 weeks of continuous use. These drugs are not approved in the EU. Examples include:
The “fat blocker” pill
Combination therapy
The reigning champion

The bonus
The bottom line
More
Do you want more?



How to lose weight - the evidence
This guide is written by Dr. Andreas Eenfeldt, MD and was last updated on June 19, 2025. It was medically reviewed by Dr. Michael Tamber, MD on May 27, 2021 and Dr. Bret Scher, MD on May 31, 2022.
The guide contains scientific references. You can find these in the notes throughout the text, and click the links to read the peer-reviewed scientific papers. When appropriate we include a grading of the strength of the evidence, with a link to our policy on this. Our evidence-based guides are updated at least once per year to reflect and reference the latest science on the topic.
All our evidence-based health guides are written or reviewed by medical doctors who are experts on the topic. To stay unbiased we show no ads, sell no physical products, and take no money from the industry. We're fully funded by the people, via an optional membership. Most information at Diet Doctor is free forever.
Read more about our policies and work with evidence-based guides, nutritional controversies, our editorial team, and our medical review board.
Should you find any inaccuracy in this guide, please email andreas@dietdoctor.com.
Researchers have found that chronic calorie restriction and dieting often fail to achieve sustainable weight loss:
Perspectives on Psychological Science 2017: Reducing calorie intake may not help you lose body weight [overview article; ungraded]
Repeated dieting attempts may actually lead to gaining more weight over time:
Obesity Reviews 2015: Pathways from dieting to weight regain, to obesity and to the metabolic syndrome: an overview [overview article; ungraded] ↩
Results from studies with higher protein diets tend to report improved weight loss and more favorable satiety hormones.
Journal of Obesity and Metabolic Syndrome 2020: Clinical evidence and mechanisms of high-protein diet-induced weight loss
[overview article; ungraded]In addition, results from studies in obese people with high insulin levels (hyperinsulinemia) suggest that lowering insulin may promote weight loss and improved insulin sensitivity:
British Medical Journal 2018: Effects of a low carbohydrate diet on energy expenditure during weight loss maintenance: randomized trial [randomized trial; moderate evidence]
Endocrinology 2017: A causal role for hyperinsulinemia in obesity [overview article; ungraded]
The Journal of Medical Practice Management 2016: Ketogenic weight loss: the lowering of insulin levels is the sleeping giant in patient care [overview article; ungraded]
↩BMJ 2020: Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials [strong evidence]
Nutrients 2017: Effects of Popular Diets without Specific Calorie Targets on Weight Loss Outcomes: Systematic Review of Findings from Clinical Trials [strong evidence]
The British Journal of Nutrition 2016: Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomized controlled trials [strong evidence]
PloS One 2015: Dietary intervention for overweight and obese adults: comparison of low-carbohydrate and low-fat diets. A meta-analysis [strong evidence]
JAMA 2014: Comparison of weight loss among named diet programs in overweight and obese adults: a meta-analysis [strong evidence]
The British Journal of Nutrition 2013: Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials [strong evidence]
↩This has been shown in meta-analyses of randomized controlled trials — considered the strongest, most robust type of evidence — comparing low-carb diets to low-fat and other diets:
Cochrane Database of Systematic Reviews 2022: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk [strong evidence]
International Journal of Endocrinology 2021: Comparing the efficacy and safety of low-carbohydrate diets with low-fat diets for type 2 diabetes mellitus patients: a systematic review and meta-analysis of randomized clinical trials [strong evidence]
Journal of Nutritional Science 2021: Restricting carbohydrates and calories in the treatment of type 2 diabetes: a systematic review of the effectiveness of ‘low-carbohydrate’ interventions with differing energy levels [strong evidence]
Current Diabetes Reports 2021: Efficacy of ketogenic diets on type 2 diabetes: a systematic review [strong evidence]
Nutrition and Dietetics 2021: Exploring the highs and lows of very low carbohydrate high fat diets on weight loss and diabetes- and cardiovascular disease-related risk markers: a systematic review [strong evidence]
BMJ 2020: Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials [strong evidence]
Nutrients 2017: Effects of Popular Diets without Specific Calorie Targets on Weight Loss Outcomes: Systematic Review of Findings from Clinical Trials [strong evidence]
The British Journal of Nutrition 2016: Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomized controlled trials [strong evidence]
PloS One 2015: Dietary intervention for overweight and obese adults: comparison of low-carbohydrate and low-fat diets. A meta-analysis [strong evidence]
JAMA 2014: Comparison of weight loss among named diet programs in overweight and obese adults: a meta-analysis [strong evidence]
The British Journal of Nutrition 2013: Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials [strong evidence] ↩
Perspectives on Psychological Science 2017: Reducing calorie intake may not help you lose body weight
[overview article; ungraded]
↩Obesity Reviews 2014: Do ketogenic diets really suppress appetite? A systematic review and meta-analysis [strong evidence] ↩
Several studies have reported that calorie intake spontaneously decreases when very few carbs are consumed:
Nutrition and Metabolism 2008:: The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus [randomized controlled trial; moderate evidence]
The American Journal of Clinical Nutrition 2008: Effects of a high-protein ketogenic diet on hunger, appetite, and weight loss in obese men feeding ad libitum [randomized controlled trial; moderate evidence]
The Journal of Medical Internet Research 2017: An online intervention comparing a very low-carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: a randomized controlled trial [moderate evidence]
In one small study, 10 obese adults with type 2 diabetes who followed a non-calorie-restricted very-low-carb diet ended up eating about 1,000 calories less, on average — even though they were permitted unrestricted intake of fat and protein foods:
Annals of Internal Medicine 2005: Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes [non-controlled study; weak evidence] ↩
Journal of the American Medical Association 2012: Effects of dietary composition during weight loss maintenance: a controlled feeding study [randomized trial; moderate evidence] ↩
British Medical Journal 2018: Effects of a low carbohydrate diet on energy expenditure during weight loss maintenance: randomized trial [moderate evidence]
Nutrients 2020: Impact of a ketogenic diet on metabolic parameters in patients with obesity or overweight and with or without type 2 diabetes: a meta-analysis of randomized controlled trials [strong evidence]
PLoS One 2020: Effect of a 90 g/day low-carbohydrate diet on glycaemic control, small, dense low-density lipoprotein and carotid intima-media thickness in type 2 diabetic patients: An 18-month randomised controlled trial [moderate evidence]
Nutrition and Metabolism 2020: Effects of weight loss during a very low carbohydrate diet on specific adipose tissue depots and insulin sensitivity in older adults with obesity: a randomized clinical trial [moderate evidence]
Obesity Reviews 2016: Impact of low-carbohydrate diet on body composition: meta-analysis of randomized controlled studies [strong evidence]
The British Journal of Nutrition 2016: Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomized controlled trials [strong evidence]
↩This is based on the consistent clinical experience of practitioners familiar with low-carb nutrition. [weak evidence] ↩
Diabetalogia 2014: Eating two larger meals a day (breakfast and lunch) is more effective than six smaller meals in a reduced-energy regimen for patients with type 2 diabetes: a randomised crossover study [moderate evidence]
PloS One 2012: Effects of meal frequency on metabolic profiles and substrate partitioning in lean healthy males [randomized trial; moderate evidence] ↩
A review of multiple high-quality studies has confirmed that following a very-low-carb ketogenic diet can significantly decrease appetite and promote natural weight loss:
Obesity Reviews 2015: Do ketogenic diets really suppress appetite? A systematic review and meta-analysis [strong evidence] ↩
In a 12-day randomized crossover study, people were allowed to eat as much as they wanted on a high-protein, normal-protein, and a low-protein diet. During the high-protein portion of the trial, they consumed 500 to 550 calories less than they did during the normal-protein and low-protein portion of the trial:
The American Journal of Clinical Nutrition 2013: Protein leverage affects energy intake of high-protein diets in humans [randomized trial; moderate evidence]
A systematic review of randomized controlled trials found that higher-protein diets tend to promote weight loss, due in part to reducing hunger and increasing satiety:
Journal of the American College of Nutrition 2004: The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review [systematic review of randomized trials; strong evidence]
Other studies show that over time, following a higher protein diet leads to less hunger than a lower protein diet. Part of this may be due to changes in hunger hormones.
The American Journal of Clinical Nutrition 2013: Contribution of gastroenteropancreatic appetite hormones to protein-induced satiety [randomized crossover trial; moderate evidence]
Nutrition Journal 2014: Effects of high-protein vs. high- fat snacks on appetite control, satiety, and eating initiation in healthy women [randomized trial; moderate evidence]
Advances in Nutrition 2015: Controversies surrounding high-protein diet intake: satiating effect and kidney and bone health [review of observational studies; weak evidence] ↩
The exact macronutrient composition may vary for each individual, but one frequently successful approach is starting with 5% of your calories from carbohydrates, 35% from protein, and 60% from fat.
This is based on the consistent clinical experience of practitioners familiar with low-carb nutrition. [weak evidence] ↩
Annual Review of Nutrition 2010: Evolutionary adaptations to dietary changes [overview article; ungraded] ↩
By far the most common sugar alcohol used in low-carb chocolate and candy is maltitol. Studies confirm that it has a high glycemic and insulin index and that a large portion is absorbed into the bloodstream:
Nutrition Research Reviews 2003: Health potential of polyols as sugar replacers, with emphasis on low glycaemic properties [overview article; ungraded]
European Journal of Clinical Nutrition 1994: Digestion and absorption of sorbitol, maltitol and isomalt from the small bowel: a study in ileostomy subjects [randomized trial; moderate evidence]
Gastroentérologie Clinique et Biologique 1991: Clinical tolerance, intestinal absorption, and energy value of four sugar alcohols taken on an empty stomach [randomized trial; moderate evidence] ↩
The Yale Journal of Biology and Medicine 2010: Gain weight by “going diet?” Artificial sweeteners and the neurobiology of sugar cravings [overview article; ungraded] ↩
Cell Metabolism 2019:
Ultra-processed diets cause excess calorie intake and weight gain: An inpatient randomized controlled trial of ad libitum food intake[randomized trial; moderate evidence] ↩Some research shows an association between eating a wide variety of different foods and abdominal weight gain, as well as greater diabetes risk:
PloS One 2015: Everything in moderation – dietary diversity and quality, central obesity and risk of diabetes [observational study; very weak evidence] ↩
Eating less often may be more beneficial when it comes to weight loss and metabolic health:
Diabetalogia 2014: Eating two larger meals a day (breakfast and lunch) is more effective than six smaller meals in a reduced-energy regimen for patients with type 2 diabetes: a randomised crossover study [moderate evidence]
PloS One 2012: Effects of meal frequency on metabolic profiles and substrate partitioning in lean healthy males [randomized trial; moderate evidence] ↩
This is based on clinical experience of low-carb practitioners and was unanimously agreed upon by our low-carb expert panel. You can learn more about our panel here [weak evidence]. ↩
Medical Hypothesis 2009: The salted food addiction hypothesis may explain overeating and the obesity epidemic [overview article; ungraded]
↩It’s often claimed that eating breakfast is good for weight control. That appears to be false:
British Medical Journal 2019: Effect of breakfast on weight and energy intake: systematic review and meta-analysis of randomised controlled trials [strong evidence]
The American Journal of Clinical Nutrition 2009: The effectiveness of breakfast recommendations on weight loss: a randomized controlled trial [moderate evidence] ↩
A review of multiple high-quality studies has confirmed that following a very-low-carb ketogenic diet can significantly decrease appetite and promote natural weight loss:
Obesity Reviews 2015: Do ketogenic diets really suppress appetite? A systematic review and meta-analysis [strong evidence]
The same is true for higher protein diets.
Obesity Reviews 2014: Protein leverage and energy intake
↩
[systematic review of randomized trials; strong evidence]Evidence-Based Physical Diagnosis (Fourth Edition) 2018: Chapter 13: Obesity [textbook; ungraded] ↩
Obesity Reviews 2014: Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis [systematic review of observational studies; moderate evidence] ↩
Nutrition Reviews 2019: Effects of carbohydrate-restricted diets on low-density lipoprotein cholesterol levels in overweight and obese adults: a systematic review and meta-analysis [strong evidence]
Diabetes Research and Clinical Practice 2018: Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: a systematic review and meta-analysis [strong evidence]
Obesity Reviews 2012: Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors [strong evidence] ↩
Obesity Reviews 2015: Pathways from dieting to weight regain, to obesity and to the metabolic syndrome: an overview [overview article; ungraded]
↩This is based on clinical experience. [weak evidence] ↩
This is based on clinical experience. [weak evidence] ↩
Diabetes & Metabolic Syndrome 2017: Induced and controlled dietary ketosis as a regulator of obesity and metabolic syndrome pathologies [randomized trial; moderate evidence] ↩
This is based on clinical experience. [weak evidence] ↩
This is based on clinical experience. [weak evidence] ↩
The following US government source shows the sugar content of many different types of fruit:
US Food and Drug Administration 2017: Raw Fruits Poster [overview article; ungraded] ↩
Nutrients 2016: Paradoxical Effects of Fruit on Obesity[overview article; ungraded] ↩
This depends to some extent on the type of fruit; for instance, berries are much lower in sugar than oranges, pineapple, bananas, and most other fruits. If someone eats 1 apple, 1 banana and 1/4 cantaloupe, the total sugar load of 55 grams will have already surpassed the sugar in one large Coke. ↩
Although study results are inconsistent, frequent beer intake has been linked to excess abdominal fat, at least in men:
Nutrition Reviews 2013: Is beer consumption related to measures of abdominal and general obesity? A systematic review and meta-analysis [Systematic review of experimental and observational studies; moderate evidence]
↩Even low-carb, low-calorie alcohols can promote weight gain. Alcohol is known to increase appetite/decrease satiety, so you may be less likely to choose healthy food and more likely to eat more. Also, alcohol competes with fats and carbohydrates for oxidation, so excessive alcohol intake can prioritize its metabolism, leading to storage of what you’re eating along with it as fat.
Nutrition Reviews 2011: Alcohol consumption and body weight: a systematic review[systematic review of cohort studies and intervention trials; weak evidence] ↩
Canadian Medical Association Journal 2017: Nonnutritive sweeteners and cardiometabolic health: a systematic review and meta-analysis of randomized controlled trials and prospective cohort studies [systematic review; moderate evidence]
PLOS Medicine 2017: Artificially sweetened beverages and the response to the global obesity crisis [overview article; ungraded] ↩
These sweeteners appear to partially activate the “food reward” pathway responsible for cravings:
The Yale Journal of Biology and Medicine 2010: Gain weight by “going diet?” Artificial sweeteners and the neurobiology of sugar cravings [overview article; ungraded]
Physiology & Behavior 2016: Recent studies of the effects of sugars on brain systems involved in energy balance and reward; relevance to low calorie sweeteners [overview article; ungraded] ↩
In this 12-week study, women assigned to drink only water lost more weight than those who drank diet sodas for 12 weeks – even though both groups followed the same weight loss plan throughout the study.
American Journal of Clinical Nutrition 2015: Effects on weight loss in adults of replacing diet beverages with water during a hypoenergetic diet: a randomized, 24-wk clinical trial [moderate evidence] ↩
These well-designed studies suggest people have an increased insulin response to food when simultaneously drinking beverages containing non-caloric sweeteners.
Diabetes Care 2013: Sucralose affects glycemic and hormonal responses to an oral glucose load [randomized trial; moderate evidence]
International Journal of Obesity 2017: Effects of aspartame-, monk fruit-, stevia- and sucrose-sweetened beverages on postprandial glucose, insulin and energy intak [randomized trial; moderate evidence]
↩Insulin therapy often promotes gain rather than loss, especially among those who are overweight or obese:
Journal of Diabetes 2017: Prediction of excessive weight gain in insulin treated patients with type 2 diabetes [randomized trial; moderate evidence] ↩
In several trials, people with type 2 diabetes have been able to discontinue or dramatically reduce their insulin dosage by eating a very-low-carb diet:
Nutrition & Metabolism 2008: The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus [randomized trial; moderate evidence]
Nutrition 2012: Effect of low-calorie versus low-carbohydrate ketogenic diet in type 2 diabetes [non-controlled study; weak evidence]
Diabetes Therapy 2018: Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: an open-label, non-randomized, controlled study [weak evidence] ↩
Diabetes Care 2012: Quantifying the effect of metformin treatment and dose on glycemic control [systematic review of randomized trials; strong evidence] ↩
Expert Opinion on Pharmacotherapy 2018: Understanding the impact of commonly utilized, non-insulin, glucose-lowering drugs on body weight in patients with type 2 diabetes [overview article; ungraded]
↩Nature Partners Journal Digitial Medicine 2019: Frequent discussion of insomnia and weight gain with glucocorticoid therapy: An analysis of Twitter posts [overview article; ungraded] ↩
Journal of Affective Disorders 1984: Weight gain. A side-effect of tricyclic antidepressants. [weak evidence] ↩
For example, Celexa (citalopram) and Zoloft (sertraline) do not appear to impact weight significantly, while Paxil (paroxetine) is known to cause weight gain.
Note that there is also some evidence that long-term use of SSRIs is associated with weight gain, but it’s not known if this is causation or just correlation:
Translational Psychiatry 2016: Is increased antidepressant exposure a contributory factor to the obesity pandemic? [overview article]
BMJ Open 2017: SSRI antidepressant use potentiates weight gain in the context of unhealthy lifestyles: results from a 4-year Australian follow-up study [very weak evidence] ↩
While the available evidence is not conclusive, studies indicate that progesterone-only birth control might result in a few kilos of weight gain, on average:
Cochrane Database Systematic Review 2016: Progestin-only contraceptives: effects on weight. [moderate evidence due to limitations of studies]
Combination contraceptives, containing both estrogen and progesterone, do not appear to have a clear or major effect on body weight:
Cochrane Database Systematic Review 2014: Combination contraceptives: effects on weight. [moderate evidence due to limitations of studies] ↩
Annals of Internal Medicine 2017: Historical perspective on the rise and fall and rise of antibiotics and human weight gain [overview article; ungraded] ↩
Physiology & Behavior 2018: Effect of sleep curtailment on dietary behavior and physical activity: a randomized crossover trial [moderate evidence]
Obesity (Silver Spring) 2017: Stress, cortisol, and other appetite-related hormones: Prospective prediction of 6-month changes in food cravings and weight [non-controlled study; weak evidence] ↩
This effect has been shown in studies of both adults and children:
Nutrients 2019: Increased hunger, food cravings, food reward, and portion size selection after sleep curtailment in women without obesity [randomized trial; moderate evidence]
Sleep 2017: Short sleep duration is associated with eating more carbohydrates and less dietary fat in Mexican American children [observational study; weak evidence]
↩Sleep medicine Reviews 2015: The role of sleep hygiene in promoting public health: A review of empirical evidence[overview article; ungraded] ↩
Obesity Reviews 2015: Do ketogenic diets really suppress appetite? A systematic review and meta-analysis [strong evidence]
Journal of Obesity and Metabolic Syndrome 2020: Clinical evidence and mechanisms of high-protein diet-induced weight loss
[overview article; ungraded] ↩When trying to trim your calories from dairy, consider foods like plain, low fat, high-protein Greek yogurt. The protein will lessen your hunger with fewer calories. ↩
According to a recent review, overweight people have been found to end up taking in more calories overall when they eat nuts – although this doesn’t seem to occur in people of normal weight:
Critical Reviews in Food Science and Nutrition 2018: Effect of nuts on energy intake, hunger, and fullness; a systematic review and meta-analysis of randomized clinical trial [strong evidence]
↩Current Obesity Reports 2021: Vitamin D and Obesity: Current Evidence and Controversies[overview article; ungraded] ↩
Nutrition Journal 2012: A 12-week double-blind randomized clinical trial of vitamin D3 supplementation on body fat mass in healthy overweight and obese women [moderate evidence]
The American Journal of Clinical Nutrition 2012: Calcium and vitamin D supplementation is associated with decreased abdominal visceral adipose tissue in overweight and obese adults [randomized trial; moderate evidence]
Clinical Nutrition 2013: Impact of vitamin D supplementation during a resistance training intervention on body composition, muscle function, and glucose tolerance in overweight and obese adults [randomized trial; moderate evidence]
↩Nutrition Journal 2012: A 12-week double-blind randomized clinical trial of vitamin D3 supplementation on body fat mass in healthy overweight and obese women [moderate evidence] ↩
International Journal of Obesity 2010: Effects of multivitamin and mineral supplementation on adiposity, energy expenditure and lipid profiles in obese Chinese women [randomized trial; moderate evidence] ↩
Several studies support the use of intermittent fasting for losing weight and providing other metabolic benefits, such as improved insulin sensitivity and lower insulin levels. IF has also been shown to be at least as good as continuous caloric restriction – and often better – when it comes to losing fat while preserving muscle:
Cureus 2018: Intermittent fasting: the choice for a healthier lifestyle [systematic review of randomized trials; strong evidence]
International Journal of Obesity 2011: The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomised trial in young overweight women [moderate evidence]
Obesity (Silver Spring) 2016: A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity [moderate evidence] ↩
Journal of Translational Medicine 2016: Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males [randomized trial; moderate evidence]
↩This is based on clinical experience of low-carb practitioners and was unanimously agreed upon by our low-carb expert panel. You can learn more about our panel here [weak evidence]. ↩
Obesity (Silver Spring) 2018: Flipping the metabolic switch: understanding and applying health benefits of fasting [overview article; ungraded] ↩
Exercise is likely good for health and wellbeing in many ways. It also has some effect on weight loss – but probably a smaller effect than most people expect:
The American Journal of Medicine 2011: Isolated aerobic exercise and weight loss: a systematic review and meta-analysis of randomized controlled trials [strong evidence for about 1-2 kilos of weight loss]
Cochrane Database of Systematic Reviews 2006: Exercise for overweight or obesity [strong evidence for about 1-1.5 kilos of weight loss]
Exercise interventions might be a bit more effective for overweight and obese adolescents (10-19 years of age):
Sports Medicine 2016: Efficacy of exercise intervention for weight loss in overweight and obese adolescents: meta-analysis and implications [strong evidence for several kilos of weight loss] ↩
Obesity 2016: Persistent metabolic adaptation 6 years after “The Biggest Loser” competition [nonrandomized study, weak evidence] ↩
Progress in Cardiovascular Diseases 2014: The role of exercise and physical activity in weight loss and maintenance [overview article; ungraded] ↩
AJCN 2019: Effect of different doses of supervised exercise on food intake, metabolism, and non-exercise physical activity: The E-MECHANIC randomized controlled trial [moderate evidence] ↩
British Journal of Sports Medicine 2017: Effects of high-intensity interval training on cardiometabolic health: a systematic review and meta-analysis of intervention studies [systematic review of randomized trials; strong evidence]
Obesity Reviews 2015: The effects of high-intensity interval training on glucose regulation and insulin resistance: a meta-analysis. [systematic review of randomized trials; strong evidence] ↩
Journal of Strength and Conditioning Research 2017: Exercise-induced hormone elevations are related to muscle growth [randomized trial; moderate evidence] ↩
This is based on clinical experience of low-carb practitioners and was unanimously agreed upon by our low-carb expert panel. You can learn more about our panel here [weak evidence]. ↩
The Journal of Nutrition 2015: A lower-carbohydrate, higher-fat diet reduces abdominal and intermuscular fat and increases insulin sensitivity in adults at risk of type 2 diabetes [randomized trial; moderate evidence]
Annals of Internal Medicine 2005: Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes [non-controlled study; weak evidence] ↩
Journal of the American Dietetic Association 2005: Perceived hunger is lower and weight loss is greater in overweight premenopausal women consuming a low-carbohydrate/high-protein vs high-carbohydrate/low-fat diet [randomized trial; moderate evidence] ↩
Current Nutrition Reports 2018: Nutritional ketosis for weight management and reversal of metabolic syndrome [overview article; ungraded] ↩
Diabetes Therapy 2018: Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: an open-label, non-randomized, controlled study [weak evidence]
↩This is based on clinical experience of low-carb practitioners and was unanimously agreed upon by our low-carb expert panel. You can learn more about our panel here [weak evidence]. ↩
Diet Doctor will not benefit from your purchases. We do not show ads, use any affiliate links, sell products or take money from industry. Instead we’re funded by the people, via our optional membership. Learn more ↩
There’s a lack of clear scientific evidence about exactly what level of protein intake is most beneficial on a keto diet.
Here are some thoughts on individualization of protein intake, and details about the views of different low-carb experts. ↩
Keep in mind that you may not be in ketosis continually during that time, but may go in and out based on other factors such as sleep, stress, exercise, and others. ↩
Diet Doctor will not benefit from your purchases. We do not show ads, use any affiliate links, sell products or take money from industry. Instead we’re funded by the people, via our optional membership. Learn more ↩
Diet Doctor will not benefit from your purchases. We do not show ads, use any affiliate links, sell products or take money from industry. Instead we’re funded by the people, via our optional membership. Learn more ↩
In hypothyroidism, metabolic rate slows down, which can lead to weight gain of about 11 pounds (5 kg):
European Thyroid Journal 2012: Thyroid function and obesity [overview article; ungraded] ↩
Best Practice & Research, Clinical Endocrinology & Metabolism 2013: Pitfalls in the measurement and interpretation of thyroid function tests [overview article; ungraded] ↩
When it comes to iodine, good sources are fish, shellfish, sea vegetables (seaweed) and iodized salt (or iodized sea salt). Do not, however, take a mega-dose iodine supplement, which can paradoxically suppress thyroid function.
Selenium is found in soil, with some regions of the world being more deficient than others. If you live in a part of the world (e.g. United States) where your food tends to get shipped to your local grocery store from geographically diverse regions, you almost certainly get enough selenium. If not, then consider supplementing your diet with Brazil nuts or other selenium-rich foods. Be careful, though, as more than 1-3 Brazil nuts per day could lead to selenium toxicity.
Iron is found in plenty of foods, but iron-deficiency is common for a multitude of reasons. If you have a history of anemia or otherwise suspect that you could be susceptible to iron deficiency, your doctor can order blood tests to investigate. ↩
Thyroid Research 2018: Management of hypothyroidism with combination thyroxine (T4) and triiodothyronine (T3) hormone replacement in clinical practice: a review of suggested guidance [overview article; ungraded] ↩
In a 6-month study, 11 women with PCOS who ate less than 20 grams of carbs per day lost 11% of their body weight, on average, along with reducing their fasting insulin levels and improving their reproductive hormone balance:
Nutrition & Metabolism 2005: The effects of a low-carbohydrate, ketogenic diet on the polycystic ovary syndrome: a pilot study [non-randomized trial; weak evidence]
A more recent study also reported excellent weight loss and other benefits of low-carb in women with PCOS:
Journal of Obesity & Weight Loss Therapy 2015: Low starch/low dairy diet results in successful treatment of obesity and co-morbidities linked to polycystic ovary syndrome (PCOS) [non-controlled study; weak evidence] ↩
BioMed Research International 2014: Estrogen Deficiency and the Origin of Obesity during Menopause[overview article; ungraded]
Diabetes, Obesity and Metabolism 2006: Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women [systematic review of randomized trials; strong evidence] ↩
Current Pharmaceutical Design 2017: Low testosterone levels and metabolic syndrome in aging male [overview article; ungraded]
↩Journal of Strength and Conditioning Research 2017: Exercise-induced hormone elevations are related to muscle growth [randomized trial; moderate evidence]
Hormone and Mteabolism Research 2011: Effect of vitamin D supplementation on testosterone levels in men [randomized trial; moderate evidence]
↩Metabolism 2018: Testosterone replacement therapy: For whom, when and how?s [overview article; ungraded]
Cochrane Database of Systematic Reviews 2017: Long-term hormone therapy for perimenopausal and postmenopausal women [systematic review of randomized trials; strong evidence]
↩Psychoneuroendocrinology 2001: Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior [randomized trial; moderate evidence]
↩Also note that a random check of blood (or salivary, or urine) cortisol during the day is often not useful, and has too much variability to tell you if cortisol is a problem for you. If you are worried about cortisol, you must focus on addressing any underlying conditions that can raise it. ↩
JAMA 2021: Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial[randomized trial; moderate evidence] ↩
The British Journal of Nutrition 2011: The efficacy of Phaseolus vulgaris as a weight loss supplement: a systematic review and meta-analysis of randomised clinical trials [strong evidence] ↩
Diabetes Therapy 2020: Drug Therapy in Obesity: A Review of Current and Emerging Treatments[overview article; ungraded] ↩
JAMA Network 2015: Efficacy of liraglutide for weight loss among patients with type 2 diabetes [randomized trial; moderate evidence] ↩
The New England Journal of Medicine 2015: A randomized, controlled trial of 3.0 mg of liraglutide in weight management [moderate evidence] ↩
International Journal of Obesity 2012: Safety, tolerability and sustained weight loss over 2 years with the once-daily human GLP-1 analog, liraglutide [randomized trial; moderate evidence] ↩
New England Journal of Medicine 2021: Once-Weekly Semaglutide in Adults with Overweight or Obesity[randomized trial; moderate evidence] ↩
This is based on the clinical experience. [weak evidence] ↩