Is your fasting blood glucose higher on low carb or keto? Five things to know

This past spring, after 18 months of great success on the keto diet, I tested my fasting blood sugar on my home glucose monitor for the first time in many months. The result shocked me.
I had purchased the device, which also tests ketones, when I was diagnosed with pre-diabetes in the fall of 2015. As I embarked on low-carb keto eating, I tested my blood regularly. Soon my fasting blood sugar was once again in the healthy range. I was in ketosis day after day. Not only that, I lost 10 lbs (5 kg) and felt fantastic — full of energy with no hunger or cravings. Before long I could predict the meter’s results based on what I was eating or doing. I put the meter away and got on with my happy, healthy keto life.
When my doctor ordered some lab tests this spring, I brought the meter out again. While I had no health complaints, excellent blood pressure and stable weight, she wanted to see how my cholesterol, lipids, HbA1c, and fasting glucose were doing on my keto diet — and I was curious, too.
To check the accuracy of my meter against the lab results, on the morning of the test I sat in my car outside the clinic at 7:30 am, and pricked my finger. I was expecting to see a lovely fasting blood glucose (FBG) of 4.7 or 4.8 mmol/l (85 mg/dl).
It was 5.8! (103 mg/dl). What? I bailed on the tests and drove home — I didn’t want my doctor warning me I was pre-diabetic again when I had no explanation for that higher result.The next morning I tested again: 5.9! (104). Huh???
For the next two weeks I tested every morning. No matter what I did, my FBG would be in 5.7 to 6.0 (102 to 106 mg/dl), the pre-diabetic range again.
One morning after a restless sleep it was even 6.2 mmol/l (113 mg/dl). But my ketones were still reading 1.5-2.5 mmol/l. I was still burning fat, not glucose. When I tested my blood after meals, my glucose hardly moved at all. My charts, which I enter at SugarStats, were almost a straight line, with the FBG the highest reading of the day, 12 to 14 hours after any food at all.
What was going on?
Many people ask: “Why is my fasting blood glucose higher on low carb?” Dozens of ketogenic and paleo forums have discussions on the issue. Some of the information flames fears, using unsubstantiated claims, that a low-carb diet could trigger diabetes rather than reverse it. Some posters in forums even say they’ve quit the keto diet because their higher FBGs scared them so much.
But have no fear. We have researched the medical literature and consulted with leading experts. Here’s what you need to know:
1. Relax, it is normal — call it “adaptive glucose sparing”
“We definitely see that in people who are doing low carb long term, the majority will find that their fasting blood glucose becomes their highest value of the day,” says Dr. Sarah Hallberg. “They are not actually having issues with blood sugar. They are doing really well. But if you are looking at a log of 24 hours of blood glucose you will see a high first thing in the morning and then a steady decline throughout the day, with no big excursions [in glucose levels] even after meals.”
The scientific name is “physiologic insulin resistance” and it’s likely a good thing — unlike “pathologic insulin resistance.”As regular visitors will know, the “pathologic” kind of insulin resistance is caused by higher and higher levels of insulin — hyperinsulinemia — trying to force glucose into our cells. That insulin resistance is a prominent feature of type 2 diabetes, polycystic ovary syndrome (PCOS) and other chronic conditions.
So let’s call physiologic insulin resistance instead “adaptive glucose sparing,” a name that has been proposed by many to reduce the confusion. Dr. Ted Naiman describes it as muscles that are in “glucose refusal mode.”
Prior to converting to the ketogenic diet, your muscles were the major sites to soak up and use glucose in the blood for energy. On a long-term keto diet, however, they now prefer fat as fuel. So the muscles are resisting the action of insulin to bring sugar into cells for energy, saying, in essence: “We don’t want or need your sugar anymore, so move it along.” Hence, the slightly elevated, but generally stable, glucose circulating in the blood.1
Where is that glucose coming from when you consume no sugar and only leafy veggie carbs in your diet? Your liver, through gluconeogenesis — the creation of glucose from non-carbohydrate sources such as lactate, glycerol, and glucogenic amino acids from proteins. It is a natural protective process that got homo sapiens through hundreds of thousands of years of feasts and famines.
“There is no essential requirement for dietary carbohydrate because humans possess a robust capacity to adapt to low-carbohydrate availability,” says Dr. Jeff Volek. In the liver of a keto-adapted person, he notes: “ketone production increases dramatically to displace glucose as the brain’s primary energy source, while fatty acids supply the majority of energy for skeletal muscle. Glucose production from non-carbohydrate sources via gluconeogenesis supplies carbons for the few cells dependent on glycolysis [using sugar for energy.]”2
Why are blood sugars highest in the morning? It’s the dawn phenomenon, when cortisol, growth hormones, adrenaline and the enzyme glucagon pulse to the liver to get you up and moving for the day — spurring gluconeogenesis for the cells that need glucose.
“It’s your body making you breakfast,” notes one post that discusses the common phenomenon — except that when your muscles are fat-adapted, they don’t want it.3
The HbA1c test estimates the average glucose level in the blood over the previous three months by counting the number of glucose molecules stuck on red blood cells. On a low-carb diet the HbA1c will almost always be lower than the fasting blood glucose suggests, showing that good glucose control, or type 2 diabetes, is not an issue for that individual.4
2. Insulin is low — an important difference
Only testing fasting blood glucose without testing fasting insulin tells you very little. That’s because two people could have exactly that same fasting blood glucose levels and have very different circulating insulin levels.5
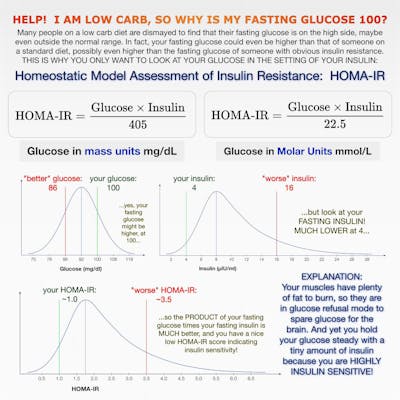
It is all about the relationship between glucose and insulin and how they work in concert. This is called the homeostatic model assessment of insulin resistance or HOMA-IR. The name is a mouthful, but it simply means that the body is always trying to keep its essential systems in balance or in an equilibrium — called homeostasis. Insulin is working against glucose in an attempt to keep blood sugar levels stable, a.k.a in homeostasis.6
In one individual — for example someone with pre-diabetes, type 2 diabetes, or PCOS — insulin may over time be pulsed out in higher and higher amounts just to keep the blood sugar relatively stable. While fasting blood glucose could still be in the normal range, it is taking increasing amounts of insulin to keep it there. As insulin resistance develops, and insulin becomes increasingly ineffective to bring blood sugars down, blood sugars will eventually rise too high.
In a second individual — someone who has been on the keto diet for a number of months and is now burning fat for energy — much lower amounts of insulin are being pulsed by the pancreas to keep the glucose stable. You have now, therefore, improved your insulin resistance and only need small amounts of insulin to keep glucose in check.
Dr. Naiman’s graph shows, if you know your fasting blood glucose and your fasting insulin, the HOMA-IR equation can tell you how insulin sensitive or insulin resistant you are. If your fasting blood sugar is 5.7 mmol/L (103 mg/dL) and your insulin is high, too, over 12 μU/mL, you are insulin resistant and may be on your way to type 2 diabetes. If your blood sugar is 5.7 mmol/L but your fasting insulin is under 9 μU/mL, you are insulin sensitive and may be in “glucose refusal” mode from a low-carb diet.
Most doctors do not yet check for fasting insulin with a fasting blood glucose test. You usually have to ask for it.7
3. Understand cortisol and its impact on blood glucose
We all live stressful lives, but some of us have a harder time reducing or releasing our stress. That fact may play out in restlessness, poor sleep, insomnia, or feelings of anxiety or constant tension. Cortisol is the stress hormone that mediates the “fight or flight” physiologic response. And it has a direct bearing on our glucose levels.
“Prolonged cortisol stimulation will raise blood glucose levels,” notes Dr. Jason Fung, who wrote an entire chapter on the stress hormone in his 2016 bestseller The Obesity Code.8 In it he describes how cortisol, released from the adrenal glands, sends a message to the body to release glucose to prepare for a perceived threat, spurring gluconeogenesis in the liver. In prehistoric times, that surge of glucose energy was usually used up fighting or fleeing from the threat. But in current days, often that stress goes unreleased, the energy not used, which can lead to prolonged higher glucose levels (and higher insulin levels to try to bring it down.)
US nurse Kelley Pound, a low-carb diabetes educator who blogs at the site LowcarbRN, wore a continuous glucose monitor to see how various foods and stimuli impacted her blood glucose throughout the day. She discovered that even while eating low carb, it was stress that had the biggest impact on her readings, far more than any low-carb food. “My blood glucose will average 20-30 points higher on mornings where I have not gotten at least 7 hours of sleep,” said Pound, who decided to focus on stress reduction as a key part of diabetes management. “Working so hard to keep blood glucose controlled with diet, only to have it go haywire with stress, is defeating my goals.”
I, too, discovered the same stress impact, especially with sleep. Since this spring, I am doing yoga in the early evening, focusing on other stress reduction activities (painting and playing my guitar at night rather than scanning Facebook or watching the news) and wearing earplugs and an eye shade to help ensure a better night sleep. Doing so drops my FBG back into the normal range the next morning.
Drinking a glass or two of wine at night can lower readings, too, because the liver metabolizes the alcohol first before turning to gluconeogenesis, but I don’t want to drink daily.
4. Glucose meters can give false readings
While physiologic reasons cause higher glucose readings, technical reasons can cause them, too. The US Federal Drug Administration allows home glucose monitors to have a variance of 15% in results. That means a reading of 100 mg/dl might actually be as low as 85 mg/dl or as high as 115, a huge variation!9
Dave Feldman, the software engineer who has cracked the Cholesterol Code, has blogged about his glucose meter variance, charting and taking pictures of his two glucose meters, measuring the same drop of blood. While he was expecting his blood glucose set point to be higher because of his long-term low-carb keto eating, he was surprised by the sometimes huge variation in results. He notes that whenever he gets an unexpected result, he takes three readings, all within a few minutes of each other, and then averages the result.
Other researchers have noted that false readings can be caused by pricking a finger for blood with hands that have minute traces of sugar or food (just touching a piece of fruit.) Dehydration raises results, too. You should always wash your hands before testing, but some soaps have additives like honey or a fragrance that can linger on fingers and distort readings. As well, strips that are too hot or too cold, or other environmental conditions like high altitudes, can produce higher or lower readings. Even different lots of strips can produce different results on the same meter.
Now, like Feldman, whenever I get an unusually high reading, I take another reading. It is often many points lower.10
5. A word about LADA – Latent Autoimmune Diabetes in Adults
If all of the information in this post does not help you understand your rising blood glucose on the low-carb diet, and your blood glucose continues to rise higher and higher, not only in the morning but at other times of day, there may be a potential issue of latent autoimmune diabetes in adults (LADA), also sometimes called type 1.5 diabetes.11
Both Dr. Hallberg and Dr. Fung say they see LADA regularly among their patients who may have been misdiagnosed with type 2 diabetes and have LADA instead.
LADA is like type 1 diabetes in that antibodies are attacking the insulin-producing cells of the pancreas, but it arises in adulthood, not in childhood or adolescence. Diabetes researchers note that LADA also has features of type 2 diabetes, but the patients usually are thinner and progress to needing insulin faster because their insulin-producing beta cells have been attacked by antibodies. The highest rates of LADA are found in Northern Europe, with up to 14% of those with type 2 diabetes actually having it.12
“I test serum C-peptide and insulin in everybody in my Intensive Dietary Management program,” notes Dr. Fung. “I re-check them over time and it often takes 6 months to 1 year to clinch the diagnosis. I would suspect about 5-10% of my type 2s are actually LADA.”
Dr. Naiman has similar experiences and routines.13
Fortunately, just like type 1 or type 2 diabetes, the low-carb keto diet is a successful way for individuals with LADA to keep their blood sugar as stable as possible. If they need to eventually inject insulin, low-carb eating enables them to use the least amount of insulin necessary to keep high blood sugars in check. “It may not slow progress of the beta cell destruction, but low carb is a very successful therapeutic strategy to reduce reliance on medication,” notes Dr. Fung.
Conclusion
After doing all this research on fasting glucose levels in low-carb keto eating, I am no longer worried about my morning highs. Now with a greater focus on stress reduction and better sleep, they are routinely in the normal range anyway, while I continue to be in ketosis and love my keto diet and keto life.
And by the way, when I finally went for the my lab test, I got great results. My lipids and cholesterol were excellent and my HbA1c was a healthy 5.3%. “Keep doing what you are doing,” my doctor said. “You are the picture of robust health.”
More
How to reverse type 2 diabetes
The dawn phenomenon – Why are blood sugars high in the morning?
Earlier
Diabetes
![My low-carb story with Marc Gossange]()
![My success story with Kenneth Russell]()
- MEMBERS ONLY
![Part 8 of Dr. Jason Fung's diabetes course]()
![A low-carb story with Dr. Sanjeev Balakrishnan]()
![Can low carb make it fun to be a doctor?]()
![How to avoid complications of type 1 diabetes]()
![Living low carb with Chris Hannaway]()
- MEMBERS ONLY
!["I have been following the wrong advice!"]()
- MEMBERS ONLY
![How to motivate your patients]()
![How to help patients reverse type 2 diabetes]()
![Living low carb with Yvonne Lane]()
- MEMBERS ONLY
![LCHF and diabetes: science and clinical experience]()
- MEMBERS ONLY
![The essential problem with type 2 diabetes]()
- MEMBERS ONLY
![How to prevent chronic disease – Dr. Trudi Deakin]()
- MEMBERS ONLY
![Diet & diabetes – how to normalize your blood sugar]()
- MEMBERS ONLY
![80 pounds lighter and no medications]()
- MEMBERS ONLY
![Why low-fat diets don't work — Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
![The science of low carb]()
- MEMBERS ONLY
![Everything goes in the right direction]()
![What's it like being a low-carb doctor on TV?]()










Dr. Fung
![Diet Doctor Podcast #64 with Jason Fung]()
- MEMBERS ONLY
![Part 8 of Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
![The essential problem with type 2 diabetes]()
- MEMBERS ONLY
![Why low-fat diets don't work — Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
![The 2 big lies of type 2 diabetes]()
- MEMBERS ONLY
![The top 5 myths of fasting]()
![Part 7 of Dr. Jason Fung's diabetes course]()
![Insulin toxicity — Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
![The cause of obesity]()
- MEMBERS ONLY
![A new paradigm for type 2 diabetes]()
![The 7 benefits of fasting]()
- MEMBERS ONLY
![Are all carbohydrates equally bad?]()
![What to do instead of counting calories]()
![The top 5 tips to make fasting easier]()
![Breakfast! Is it really that important?]()
- MEMBERS ONLY
![The most common questions]()
![The perfect treatment for diabetes and weight loss]()
![How to fast - the different options]()
![Therapeutic fasting]()
- MEMBERS ONLY
![The key to obesity]()









Dr. Hallberg
![How to help patients reverse type 2 diabetes]()
![A low-carb diet for T2D reversal – Dr. Sarah Hallberg]()
![Reverse diabetes by ignoring the guidelines]()
![Is high cholesterol dangerous on a low-carb diet?]()
![Diet Doctor podcast #10 with Dr. Sarah Hallberg]()
![LCHF and LDL]()
- MEMBERS ONLY
![Cooking keto with Dr. Sarah Hallberg]()





Dr. Naiman
- MEMBERS ONLY
![Why more protein is better]()
![Is obesity caused by too much insulin?]()
![Bodyweight training for beginners with Dr. Ted Naiman]()
![Diet Doctor Podcast #40 with Ted Naiman]()
- MEMBERS ONLY
![What causes insulin resistance?]()
- MEMBERS ONLY
![Hyperinsulinemia - what insulin does in your body]()
![Becoming a low-carb doctor]()
![Too much protein is better than too little]()



Metabolism: Metabolic characteristics of keto-adapted ultra-endurance runners ↩
Heads Up Health: Low-carb lab testing – Part 2 – Fasting insulin test ↩
Heads Up Health: Low-carb lab testing – Part 2 – Fasting insulin test ↩
Diet Doctor will not benefit from your purchases. We do not show ads, use any affiliate links, sell products or take money from industry. Instead we’re funded by the people, via our optional membership. Learn more ↩
FDA: Self-monitoring blood glucose test systems for over-the-counter use ↩
- Diabetes Technology & Therapeutics: System accuracy of blood glucose monitoring systems: impact of use by patients and ambient conditions
- Journal of Diabetes Science and Technology: Interferences and Limitations in Blood Glucose Self-Testing
World Journal of Diabetes: Latent autoimmune diabetes in adults: A distinct but heterogeneous clinical entity ↩
Diabetic Medicine: Latent autoimmune diabetes of the adult: current knowledge and uncertainty ↩
Dr. Naiman’s comment on the topic:
↩Yes I have definitely diagnosed LADA and have patients who have used low carbohydrate diets to manage it… have one LADA patient who required insulin during a pregnancy prior to low carb diet but now is able to stay off medication as long as she is very careful with diet. Insulin production is low but not so low that she has to use insulin. I do routinely check antibodies in almost all adults with a new diabetes diagnosis, as well as insulin levels (or c-peptide if they are on insulin) because I want to know the following about all my patients with diabetes:
• do they have insulin RESISTANCE, and if so how much
• do they have insulin DEFICIENCY, and if so how much
• do they have an autoimmune component, and is it worsening over time