The difficulties of diagnosing PCOS – PCOS 4

Making the diagnosis of PCOS in adolescents is particularly tricky. When girls first begin to menstruate (called menarche), cycles are commonly irregular and may not always be accompanied by ovulation. In the United States, the median age of menarche is 12.4 years. This period of irregular cycles often lasts for 2 years or more, and cycle intervals typically range from 21-45 days (average 32.2 days). This is quite close to the 35 day cycles defined as oligomenorrhea.
Thus, normal puberty and the irregular cycles seen in PCOS overlap significantly. Over-diagnosis in this age group may lead to over-treatment and unnecessary worry. By the third year after menarche, 60-80% of cycles are 21-34 days long, typical of normal adult cycles, making the distinction easier.
During puberty, there is a normal physiologic increase in testosterone levels that peaks a few years after menarche. Blood testing does not distinguish unusually high levels because normal levels are not well defined in adolescents. This increased testosterone, for example, leads to the familiar problem of acne during teenage years that improves or disappears in later adult years. This temporary stage of increase in acne does not predict later disease.

Acanthosis nigricans is seen as a velvety dark patch, usually on the neck or body folds. This clinical finding is common in people and is considered characteristic of high insulin resistance and often found in patients with type 2 diabetes. The severity of acanthosis nigricans is directly related to the severity of insulin resistance. The higher the insulin resistance, the bigger and darker the skin patches.
Polycystic ovaries too, are difficult to diagnose during adolescence. Trans-vaginal ultrasound (where the ultrasound probe is inserted into the vagina) provides the clearest images of the ovary. However, this is usually avoided in adolescent girls, making the radiologic diagnosis more difficult. Nevertheless, in the studies performed, 26-54% of asymptomatic adolescent girls have polycystic ovaries by imaging.
The three criteria used for diagnosis of PCOS – hyperandrogenism, irregular cycles and polycystic ovaries can all be found during normal puberty. Special care must be taken in labelling a patient with PCOS, and it is often prudent to wait until after adolescence to make the diagnosis since this is not an urgent condition to treat. Obviously, if there is evidence of type 2 diabetes or obesity, these associated conditions should be treated.
Obesity itself is known to be associated with increased insulin levels. This effect is magnified during early puberty. During Tanner stage 3 (early puberty) for example, 93.8% of obese pre-teens have elevated testosterone versus 0% of non-obese. Fasting insulin is over three times higher in the obese group. This effect is also seen during late puberty and adulthood, but there is not such a marked difference.
Differential diagnosis
Hyperandrogenism and polycystic ovaries are not exclusive to PCOS, so other diseases that mimic PCOS must be excluded. While these conditions are rare, they may be serious and require entirely different treatments, so making the distinction is important. The list of similar conditions includes:
- Pregnancy
- Prolactin excess
- Thyroid disease
- Adrenal hyperplasia
- Cushing’s Syndrome
- Androgen-producing tumors
- Drug-induced
PCOS can only be diagnosed when these other problems have been excluded by history, physical or laboratory examination. Let us consider some of these other conditions.
Pregnancy
Pregnancy is, by far the most common cause of menstrual irregularity. Obviously, a simple pregnancy test, either a home test or laboratory confirmation is mandatory in the workup of PCOS. It would be very embarrassing to miss this simple diagnosis.
Hyperprolactinemia
Hyperprolactinemia is the presence of an excess of the hormone prolactin in the blood. Prolactin is normally secreted by the pituitary gland in the brain that enables mammals, including humans, to produce milk. Prolactin increases normally towards the end of pregnancy for proper breast development.
A wide range of conditions may lead to hyperprolactinemia, including chronic kidney or liver disease, drugs, and thyroid disease. Another common disease is a small tumor (micro-adenoma) of the pituitary gland may over-secrete prolactin into the blood. The diagnosis is made by measuring prolactin blood levels.
High prolactin levels may inhibit estrogen and cause menstrual irregularities and difficulty with ovulation. This may mimic the presenting symptoms of PCOS. Other symptoms that may help differentiate the disease include breast enlargement and abnormal milk production.
Thyroid disorders
The thyroid is a small gland at the front of the neck. It secretes thyroid hormone which controls many aspects of metabolism. Disorder of too little thyroid hormone may cause weight gain, menstrual irregularities, infertility and hair loss that may be confused with PCOS. Blood testing of thyroid hormones (TSH, T3, T4) should be performed to rule out this easily treated condition.
Non-classic congenital adrenal hyperplasia (NCAH)
NCAH is a rare genetic disorder presenting with clinical features of hyperandrogenism similar to PCOS,often in young girls and women. Androgens are normally produced in both the ovaries and the surface (cortex) of the adrenal glands. Rarely, NCAH causes overproduction of androgens by the adrenal glands and a syndrome reminiscent of PCOS, with irregular menstruation, hirsutism and acne. Blood tests, specifically the 17-OH-PG response to ACTH stimulation will distinguish between NCAH and PCOS.
Cushing’s syndrome
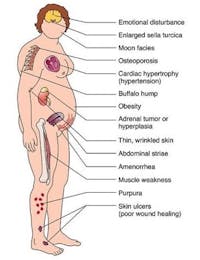
Prolonged exposure to high levels of a hormone called cortisol causes Cushing’s Syndrome. In some cases, tumors may over-secrete cortisol. In other cases, synthetic cortisol (prednisone) is used as a medication for the treatment of autoimmune diseases (asthma, lupus) and in transplantation to suppress the immune system. Elevated cortisol levels can cause weight gain, menstrual irregularities and infertility which may be confused with PCOS.
The presence of other symptoms such as characteristic fat distribution (buffalo hump), striae, thinning of skin, muscle weakness and atrophy, sensitivity to infections, decrease in bone density and severe psychiatric and cognitive dysfunction, may help distinguish this from PCOS. Blood testing can detect the high cortisol levels which will differentiate this from PCOS.
Androgen excess (drug/tumour induced)
Tumors in the adrenal glands or ovaries may over-secrete androgens causing hirsutism, clitoral enlargement, deepening of the voice, and male pattern baldness. These are extremely rare, but potentially life threatening. The average age of diagnosis is 23.4 years, overlapping significantly with PCOS. Tumors typically produce far higher levels of androgen than are found in PCOS, leading to far more severe symptoms. Imaging such as abdominal CT scanning may be necessary to find such tumors.
Drug induced androgen excess may be found in those surreptitiously taking testosterone, mostly for athletic performance. Because patients may not always admit to their use, a high index of suspicion is necessary to make the diagnosis.
Epidemiology
Using the NIH 1990 criteria, the prevalence of PCOS ranges from 6-9%, with a strikingly similar rate throughout the world despite wide disparity in the rates of obesity. When using the broader Rotterdam criteria, PCOS prevalence is generally double that of using the older NIH criteria. Thus, most newer estimates of the prevalence suggest it affects 15-20% of women, making it the most common endocrine disorder of young women by far. Approximately 1 in 15 unselected women in the United States are affected with similar proportions in Spain, Greece and the United Kingdom. This suggest that an estimated 105 million women are thus afflicted.
Twin studies show that there is a clear genetic influence on fasting insulin levels, body mass index and androgen levels. A large Dutch study comparing identical twins to fraternal twin sets, found that approximately 70% of PCOS may be attributed to genetic influences. This is comparable to the estimated 70% of obesity that may be related to genetics. Thus, it is likely that genes influence the overall predisposition to both obesity and PCOS.
Both obesity and PCOS runs in families. Sisters of PCOS patients are more likely to have symptoms with an estimated 22% also fulfilling the full diagnostic criteria. A further 24% of sisters had hyperandrogenism but regular menstrual cycles, likely indicating that they, too likely had mild PCOS. Mothers of patients with PCOS had higher androgen levels, insulin resistance and metabolic syndrome. First degree relatives, male or female are more likely to have evidence of insulin resistance. Despite these strong genetic tendencies, no single gene has been identified as the causative factor indicating that PCOS is a complex genetic disorder with multiple genes contributing small degrees of risk.
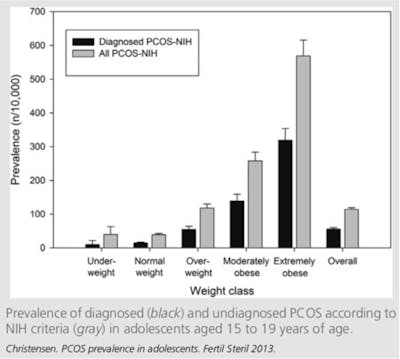
In addition to the human suffering, the economic burden of PCOS is huge. In the United States, an estimated $4 billion in 2004 was spent on health care related costs. PCOS is one of the leading causes of infertility and in vitro fertilization, a multi-billion dollar industry. Women with PCOS who do become pregnant are at increased risk of obstetrical complications such as gestational diabetes, pregnancy induced hypertension and pre-eclampsia.PCOS is associated with many diseases that do not form part of the diagnostic criteria. Perhaps the most important is a history of weight gain that often precedes the diagnosis of PCOS. 28.3% of obese women referred to one clinic were diagnosed with PCOS Weight loss has also been proven to reduce testosterone, improve insulin resistance and decrease hirsutism (more on this later). PCOS is more common with increasing severity of obesity, but the effect is quite modest.
It is also recommended to routinely screen for type 2 diabetes. Measuring fasting glucose alone may miss the diagnosis of up to 80% of pre-diabetic patients and 50% of diabetic patients. This misses an opportunity to pick up the disease at an early stage and intervene with lifestyle measures and prevent end organ damage. Current guidelines recommend that women with PCOS should be screened using an oral glucose tolerance test every 3-5 years. If there are other risk factors, this should be done annually.
Other important considerations are to assess for cigarette smoking and for psychological wellbeing. Both depression and anxiety are common among PCOS patients and a high index of suspicion should be maintained.
Patients with PCOS have double the chance of being hospitalized compared to those without the disease. PCOS is associated with obesity, type 2 diabetes, high blood pressure, and stroke. The increased type 2 diabetes and metabolic syndrome puts women at high risk later in life from heart disease, strokes and cancer. Therefore, this $4 billion bill is likely a significant underestimation of the total fiscal cost of this disease, which pales in comparison to the human suffering. By comparison, this is three times the total cost of hepatitis C, another significant public health issue.
In trying to understand the proper treatment of PCOS, it is necessary to understand the underlying cause of disease. With its close links to obesity and type 2 diabetes, PCOS has clearly emerged as a disease of metabolism, rather than simply a reproductive disorder, so understanding the link to obesity is the best place to start.
Dr. Fung’s top posts
![Longer fasting regimens – 24 hours or more]() Longer fasting regimens – 24 hours or more
Longer fasting regimens – 24 hours or more![How to renew your body: Fasting and autophagy]() How to renew your body: Fasting and autophagy
How to renew your body: Fasting and autophagy![My single best weight loss tip]() My single best weight loss tip
My single best weight loss tip



Weight loss
![My success story with Kenneth Russell]()
![My success story with Chuck Hicks]()
- MEMBERS ONLY
![How to motivate your patients]()
![My success story with Jim Caldwell]()
- MEMBERS ONLY
![The hidden costs of medications]()
![Living low carb with Yvonne Lane]()
- MEMBERS ONLY
![Living low carb: Sue Jones and Michael]()
![Are all calories the same?]()
![Diet Doctor Podcast #35 with Ben Bikman, PhD]()
![Pie-making champion goes low carb]()
- MEMBERS ONLY
![Will a low carb diet shorten your life?]()
- MEMBERS ONLY
![Q&A with Franziska Spritzler]()
- MEMBERS ONLY
!["I'll do this or I'm going to die trying"]()
- MEMBERS ONLY
![200 pounds lost and a health journey for the family]()
- MEMBERS ONLY
![80 pounds lighter and no medications]()
- MEMBERS ONLY
![The science of low carb]()
- MEMBERS ONLY
![Everything goes in the right direction]()
- MEMBERS ONLY
![He questioned his own beliefs]()
- MEMBERS ONLY
![Q&A with Dr. Eric Westman]()
!["It was so incredibly easy!"]()
- MEMBERS ONLY
![Why a low-carb diet and other questions]()
![What's it like being a low-carb doctor on TV?]()
![Is obesity caused by too much insulin?]()
- MEMBERS ONLY
![Weight loss and type 2 diabetes reversal on low carb – is it sustainable?]()









Keto
- MEMBERS ONLY
![Eating keto to survive cancer]()
![All things keto with Keto Connect]()
- MEMBERS ONLY
![Exploiting cancer metabolism with ketosis]()
![My success story with Jim Caldwell]()
- MEMBERS ONLY
![A new life with a keto diet]()
- MEMBERS ONLY
![Treating cancer with a keto diet]()
- MEMBERS ONLY
![LCHF and diabetes: science and clinical experience]()
![Diet Doctor Podcast #35 with Ben Bikman, PhD]()
- MEMBERS ONLY
![A life without migraines]()
- MEMBERS ONLY
![Challenging the dogma]()
- MEMBERS ONLY
!["I'll do this or I'm going to die trying"]()
- MEMBERS ONLY
![80 pounds lighter and no medications]()
![Diet Doctor Podcast #31 – Dr. Ken Berry]()
- MEMBERS ONLY
![Low-carb living]()
![My success story with Gillian Szollos]()
- MEMBERS ONLY
![Q&A with Miriam Kalamian]()
- MEMBERS ONLY
![Is lower insulin the key to better brain health?]()
- MEMBERS ONLY
![Trouble shooting high blood-glucose levels]()
- MEMBERS ONLY
![How to reverse type 2 diabetes]()
- MEMBERS ONLY
![Can you treat cancer with low carb?]()
- MEMBERS ONLY
![Is fear of protein the new fear of fat?]()
- MEMBERS ONLY
![Low-carb living]()
- MEMBERS ONLY
![How to formulate a low-carb keto diet]()
- MEMBERS ONLY
![Low-carb ketogenic diets for athletes]()












Intermittent fasting
- MEMBERS ONLY
![The 2 big lies of type 2 diabetes]()
- MEMBERS ONLY
![The top 5 myths of fasting]()
- MEMBERS ONLY
![The cause of obesity]()
![The 7 benefits of fasting]()
![What to do instead of counting calories]()
![The top 5 tips to make fasting easier]()
![Breakfast! Is it really that important?]()
- MEMBERS ONLY
![The most common questions]()
![The perfect treatment for diabetes and weight loss]()
![How to fast - the different options]()
![Therapeutic fasting]()
- MEMBERS ONLY
![Q&A about low carb & fasting]()
![The power of a 7-day fast]()
![How to get started with fasting]()
- MEMBERS ONLY
![Clinical use of therapeutic fasting]()
- MEMBERS ONLY
![Can fasting be problematic for women?]()
![Diet Doctor Podcast #23 – Dr. Jason Fung]()
![What is fasting?]()
![Understanding and treating type 2 diabetes – Dr. Jason Fung]()
![How to maximize fat burning]()
![Diet Doctor Podcast #4 with Joseph Antoun]()
![Coaching Intermittent Fasting – Diet Doctor]()














More with Dr. Fung
Dr. Fung has his own blog at idmprogram.com. He is also active on Twitter.
Dr. Fung’s books The Obesity Code, The Complete Guide to Fasting and The Diabetes Code are available on Amazon.