“It’ll cost you a quarter” – Measuring the effect of carbohydrate restriction in the hospital

“It’ll cost you a quarter,” she said every time I asked to examine her – a woman in her 80’s who was admitted to the hospital for a complicated infection related to a recent procedure that would require another surgery and, unfortunately, another one after that.
“My kind of patient, though,” I thought, appreciating that her sense of humor was intact despite the circumstances, and indeed I was right. Not only was she a delight to interact with on a daily basis, but also she was a perfect example of the impact carbohydrate restriction can have on the control of diabetes in the hospital.
She came across initially as an ornery old woman, but I never let that bother me. Establishing rapport with patients can be difficult for hospitalists because of the unique circumstances of the clinical encounters that take place in an acute facility. In contrast to an outpatient physician who can get to know patients over the course of many visits, hospitalists are often in the position of delivering bad news and discussing big decisions upon first encountering a patient, with little time to learn about the other person or develop an understanding of how things will work with each other.
This situation was no different. In addition to explaining the anticipated complex treatment plan for her infection, I also felt compelled to tell her how badly the medical system has failed her over the past 40+ years in regards to her chronic illnesses. She had had type 2 diabetes mellitus (DM) for many years complicated by chronic kidney disease (CKD), coronary artery disease (CAD), and congestive heart failure (CHF). In addition, she was morbidly obese and suffered from hypertension (HTN) and severe arthritis. Everything about her screamed “Insulin Resistance” to me, by her chart and in person.
As she was so frustrated by the complication of her recent surgery and the need to be back in the hospital, however, I felt that my first encounter with her may not be the right time to delve into my standard presentation about the role of nutrition in the management of diabetes. I would be back early in the morning and would ensure there was plenty of time to discuss these issues.
“What else do you recommend, doc?” she implored.
Perhaps I misjudged her. Or perhaps she could tell I was holding back. No matter… I was ready.
I gave her an honest assessment of her metabolic health – quite frankly, it was a smoldering disaster. She’d been developing complications of diabetes for decades, and everyone acted like this progression of disease was some immutable law of the universe, content with her being dependent on multiple medications to handle each one of her diagnoses. She agreed with my assessment of these unfortunate circumstances and offered her own critique of her declining health.
Advice to restrict carbohydrates
Ultimately, I advised a real-food, low-carbohydrate diet – to be embraced with a life-or-death seriousness. At her age, she didn’t have time to ease into the lifestyle; she needed dramatic change in her metabolic health immediately. If she was to stand any chance of eradicating this infection, she needed her glucoses under control. As I explained, elevated glucoses provide fuel to bacterial infections just as gasoline does to a fire. Infections in the setting of uncontrolled diabetes are quite problematic and simply do not respond well to standard treatment regimens.
She listened to my reasoning and assured me that she would give carbohydrate restriction a try, since the basic concept made perfect sense to her. She admitted then that she had even contemplated giving up by not having the surgery, which would have guaranteed a gradual demise as well as complete dependence on others due to her current bedridden state. Understandably, she was tired from her recent surgery and just couldn’t fathom going through rehab again. She appreciated the idea, however, that surgery at least gave her a chance at being functional again.
Perhaps more importantly, though, she loved the idea that simply changing her diet back to the way she knew her parents and grandparents to eat could have a very favorable impact on her health. She vividly recalled the days when her family always knew where their food came from. The value of real food, however, slowly degraded over the ensuing decades, and her health followed. Now, for the first time in her adult life, someone had just empowered her with a realistic tool that could allow her to take back her health that had suffered for so long.

After some encouragement that her situation was not hopeless and that she still had the power to make a difference, she decided to proceed with surgery and truly made a good-faith effort towards restricting carb intake.
Effect of carbohydrate restriction
This case serves as an excellent demonstration of the benefits of carbohydrate restriction that I routinely witness in the hospital. This effect was reinforced by the fact that my patient had been admitted to the hospital one day prior to my first encounter with her and had been initially started on the standard “diabetic” diet allowing 60 grams of carbohydrates per meal, 3 times daily. Her glucose was consistently above 150 mg/dL (8.3 mmol/L), and she was given sliding-scale insulin each time (a dose of rapid-acting insulin given before/at meals that is dosed based on the glucose level, most commonly 2 units of insulin for every 50 mg/dL over 150 mg/dL).
Here’s what happened after my low-carb intervention:
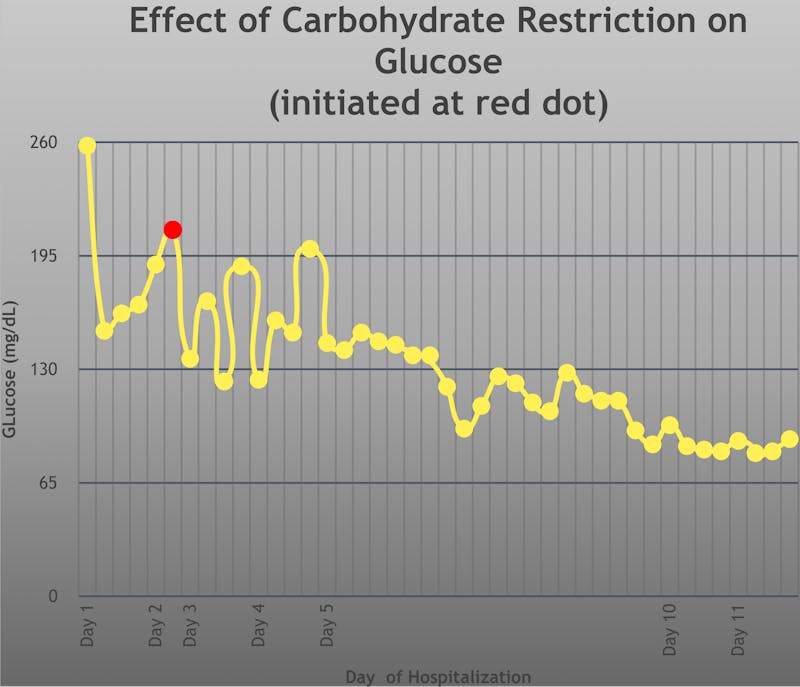
The red dot indicates when I initiated the 45-gram carbohydrate restriction and advised her that eating as few carbs as possible was the ideal way to improve her glucoses. Within 3 days, there was marked improvement in the variability of glucose readings and a strong trend toward improved glycemic control. Furthermore, she didn’t require any insulin from that point on. Within 8 days after starting carbohydrate restriction, her pre-meal glucoses had normalized at less than 100 mg/dL (5.5 mmol/L)… all without insulin.
Carbohydrate restriction works
These results are typical – I witness this rapid improvement in glycemic control on a daily basis. This particular case was chosen to illustrate the effectiveness of carbohydrate restriction because of the extent of the data available to me, from both before my intervention and for several days after. Thankfully, though, most patients do not require hospitalization for so many days.
At the completion of my work week, this patient was still hospitalized, awaiting the 2nd surgery and excelling at controlling her diabetes with her new low-carb lifestyle. Though there were a multitude of factors that would ultimately determine her response to treatment, I can be reassured that her diabetes was no longer an active complicating factor. As a result of improved glycemic control, she was given a remarkably better chance at overcoming the infection.
The results speak for themselves: carbohydrate restriction improves glycemic control. In a little over a week, my patient normalized her glucoses with a simple intervention that was quick, safe (no need for insulin or other drugs), and free (no added cost). This treatment modality has the power to transform diabetes care in the hospital. While it certainly helps to have the buy-in and support of hospital staff to achieve similar results, it can be done anytime and anywhere. All it took was an eye-opening discussion between doctor and patient.
Feeling a bit guilty about not carrying quarters to “pay” my patient for the daily exams, I handed her a dollar bill on my 4th visit. She politely refused. She thanked me, however, for the new positive outlook she had. Gone were the days that she felt hopeless about managing her diabetes and associated conditions. Now, she had her eyes set on a full recovery and on continuing to conquer diabetes with real food. With results like that, I’d happily pay a quarter every day.
More
How to reverse type 2 diabetes
Success stories
![My low-carb story with Marc Gossange]()
![My success story with Kenneth Russell]()
![A low-carb story with Dr. Sanjeev Balakrishnan]()
![Living low carb with Chris Hannaway]()
- MEMBERS ONLY
!["I have been following the wrong advice!"]()
![Living low carb with Yvonne Lane]()
- MEMBERS ONLY
![80 pounds lighter and no medications]()
- MEMBERS ONLY
![Everything goes in the right direction]()
- MEMBERS ONLY
![Carbs or not for type 1 diabetics?]()
- MEMBERS ONLY
![Living low carb with John Holding]()
- MEMBERS ONLY
!["I knew nothing"]()
- MEMBERS ONLY
![Get off the type 1 diabetes roller coaster]()
![A revolutionary treatment of type 1 diabetes]()
![Improve type 1 diabetes with low carb]()
![My success story with Mitzi Champion]()
- MEMBERS ONLY
!["How are you doing this?"]()
- MEMBERS ONLY
![Losing weight and reversing diabetes]()
![A heart attack became their wake-up call]()












Diabetes
![My low-carb story with Marc Gossange]()
![My success story with Kenneth Russell]()
- MEMBERS ONLY
![Part 8 of Dr. Jason Fung's diabetes course]()
![A low-carb story with Dr. Sanjeev Balakrishnan]()
![Can low carb make it fun to be a doctor?]()
![How to avoid complications of type 1 diabetes]()
![Living low carb with Chris Hannaway]()
- MEMBERS ONLY
![How to motivate your patients]()
- MEMBERS ONLY
!["I have been following the wrong advice!"]()
![How to help patients reverse type 2 diabetes]()
![Living low carb with Yvonne Lane]()
- MEMBERS ONLY
![LCHF and diabetes: science and clinical experience]()
- MEMBERS ONLY
![The essential problem with type 2 diabetes]()
- MEMBERS ONLY
![How to prevent chronic disease – Dr. Trudi Deakin]()
- MEMBERS ONLY
![Diet & diabetes – how to normalize your blood sugar]()
- MEMBERS ONLY
![Why low-fat diets don't work — Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
![80 pounds lighter and no medications]()
- MEMBERS ONLY
![The science of low carb]()




Top videos with low-carb doctors
- MEMBERS ONLY
![Part 8 of Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
!["Humans are not broken by default"]()
![Can low carb make it fun to be a doctor?]()
![How to help patients reverse type 2 diabetes]()
- MEMBERS ONLY
![Tim Noakes on trial]()
- MEMBERS ONLY
![The human body needs good saturated fats — Dr. Ken Berry]()
- MEMBERS ONLY
![LCHF and diabetes: science and clinical experience]()
- MEMBERS ONLY
![Launching the Diet Doctor podcast]()
- MEMBERS ONLY
![Challenging the dogma]()
![A global food revolution]()
![Diet Doctor Podcast #26 – Dr. Ignacio Cuaranta]()
- MEMBERS ONLY
![Why more protein is better]()
![Diet Doctor Podcast #36 with Eric Westman]()
- MEMBERS ONLY
![How to prevent chronic disease – Dr. Trudi Deakin]()
- MEMBERS ONLY
!["I make a difference every day"]()
![A low-carb story with Dr. Campbell Murdoch]()
- MEMBERS ONLY
![He questioned his own beliefs]()
- MEMBERS ONLY
![Weight loss and type 2 diabetes reversal on low carb – is it sustainable?]()