Why type 2 diabetes is a reversible dietary disease

Diabetes associations repeatedly tell the story that type 2 diabetes is a chronic and progressive disease. It is inevitable, like getting older. As much as we would like to stop the process, it is impossible. There is no hope to change its course. It cannot be prevented and cannot be reversed.
However, multiple studies and common sense conclusively show that this assertion is false. It is only a carefully crafted deception.
In 1986, the World Health Organization helped to fund the China Da Qing Diabetes Prevention Outcomes Study, a randomized controlled trial of lifestyle interventions lasting over twenty years. During the first six years of active intervention of diet and exercise, the incidence of diabetes was reduced by 43%. This benefit persisted over the extended follow up period of twenty years. Onset of type 2 diabetes had been delayed by an average of 3.6 years with diet and exercise.
Similar randomized, controlled studies of lifestyle interventions have shown exactly the same benefit around the world. In the United States, the Diabetes Prevention Program reduced the incidence of type 2 diabetes by 58% while maintaining an average weight loss of 5% over 4.8 years. Ten-year follow up continued to show a substantial 34% benefit. The Indian Diabetes Prevention Programme used lifestyle modifications to reduce the incidence of type 2 diabetes by almost 30%. The Finnish Diabetes Prevention Program reported a 58% reduction. A Japanese trial was able to reduce progression by 67%.
The one factor of over-riding importance to note is that all these successful prevention studies use lifestyle changes. Type 2 diabetes is overwhelmingly a lifestyle disease, so lifestyle interventions are required, not medications. You can’t use drugs to prevent a dietary disease.
Type 2 diabetes is not chronic and progressive. It is preventable. But can it be reversed?
Lessons from bariatric surgery
Far too many diabetes specialists, doctors and researchers believe that type 2 diabetes is a chronic and progressive disorder. Once you have type 2 diabetes, it will eventually get worse, no matter what you do. No amount of dietary or lifestyle change will alter the natural course of this disease, so you may as well accept it. Medications may help manage the disease but there is no hope of actually curing or reversing type 2 diabetes.
This message of despair is found everywhere. The American Diabetes Association proclaims point-blank on its website that, “Fact: For most people, type 2 diabetes is a progressive disease”. Diabetes Australia carries a similar despondent message for patients. It says, “Over time most people with type 2 diabetes will also need tablets and many will also need insulin. It is important to note that this is just the natural progression of the disease”.
 These organizations, supposed to represent the interests of people with diabetes, all pronounce that progression of this disease is both natural and normal. ‘Progression’ here is a euphemism for the blindness, kidney failure, amputations, infections, heart attacks, cancer and stroke that accompany late stage type 2 diabetes. With this message, the health professionals spread learned helplessness to patients. “Abandon hope, all ye who enter”, they roar.
These organizations, supposed to represent the interests of people with diabetes, all pronounce that progression of this disease is both natural and normal. ‘Progression’ here is a euphemism for the blindness, kidney failure, amputations, infections, heart attacks, cancer and stroke that accompany late stage type 2 diabetes. With this message, the health professionals spread learned helplessness to patients. “Abandon hope, all ye who enter”, they roar.
But there is a major problem with these edicts of hopelessness. They are simply not true. They are only lies. Type 2 diabetes is actually a reversible, curable dietary disease. Further, I can prove it to you quite easily.
Bariatric surgery
Bariatric surgery is devoted to developing procedures designed to help patients lose weight. The earliest endeavor to surgically cure obesity was to simply wire the jaws shut. The logic is obvious, if not very imaginative. This treatment though was ultimately unsuccessful. Patients could still drink fluids, and enough high calorie sugary drinks derailed weight loss. Dental infections and vomiting were also insurmountable problems.
Dr. Payne ushered in the modern age of weight loss surgery in 1963 with the jejuno-colic bypass operation. He had developed this operation after observing that patients who lost their small bowel for other reasons, such as trauma or tumors, would lose significant amounts of weight. The stomach is untouched, but instead, the small bowel, which absorbs most of the ingested nutrients, is completely bypassed. Food was rerouted from the stomach directly to the colon. As expected, patients lost significant amounts of weight.
But side effects and operative problems became immediately obvious. Patients developed night blindness from Vitamin A deficiency, and osteoporosis from Vitamin D deficiency. Severe diarrhea and bacterial overgrowth, liver failure, and kidney stones were also common. Continual diarrhea from the mal-absorbed fat led to anal excoriations and hemorrhoids. No fun. Severe complications forced the switch in 1969 to the less intensive jejuno-ileal bypass. Even still, complications were not acceptable and this surgery is now simply a historical footnote. However, other surgeons were able to build upon its initlal success.
There are two general types of weight-loss surgery, mal-absorptive and restrictive. Mal-absorptive surgeries alter the intestines so that ingested food is not properly absorbed. Dr. Payne’s early jejuno-ileal bypass is an example of a purely mal-absorptive type of surgery. Restrictive types of surgery place some obstacle to prevent food being eaten.
Earlier, in 1925, a report in the Lancet had chronicled that patients with partial removal of the stomach for peptic ulcer disease often demonstrated permanent weight loss and complete resolution of sugar in the urine, now known to be diabetes. Similar reports followed sporadically in the 1950s and 1960s. In 1967, surgical success improved when a restrictive component was added to conventional bariatric surgery.
In addition to the partial bypass of the small bowel, part of the stomach was removed as well. With the basic idea in place, further refinements were added over time, leading to the present day Roux-en-Y bypass surgery, which is still considered the most powerful weight loss surgery available. Some 140,000 such surgeries were performed in the United States in 2005.
Different types of surgery
 In the Roux-En-Y surgery, most of the healthy stomach is removed until the only portion remaining is approximately the size of a walnut. This severely restricted the amount of food that could be comfortably eaten. The second step of the surgery was to rewire the small intestines so that any ingested food could not be properly absorbed. Because this is a combined restrictive and mal-absorptive surgery, it tends to be more powerful than simpler surgeries that target only one pathway. It is also associated with far more complications, but does tend to work well for weight loss, as you may well imagine.
In the Roux-En-Y surgery, most of the healthy stomach is removed until the only portion remaining is approximately the size of a walnut. This severely restricted the amount of food that could be comfortably eaten. The second step of the surgery was to rewire the small intestines so that any ingested food could not be properly absorbed. Because this is a combined restrictive and mal-absorptive surgery, it tends to be more powerful than simpler surgeries that target only one pathway. It is also associated with far more complications, but does tend to work well for weight loss, as you may well imagine.
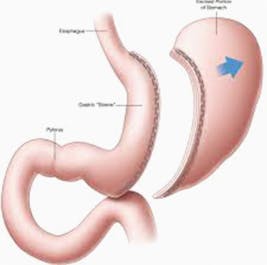
Because of the complexity and complications of the Roux-En-Y procedure, simpler forms of surgery have since been invented. A popular recent surgery is called the sleeve gastrectomy. A large portion of the healthy stomach is simply removed with none of the intestines being surgically altered. This is a purely restrictive form of weight-loss surgery. Results were not quite as good as the Roux-en-Y, but still nevertheless very good.
 The stomach’s capacity for holding food is reduced so much that it is often impossible to eat. A liquid diet is often necessary in the postoperative period. Eating any more than a thimbleful will result in severe gastric distention, ballooning of the miniature stomach. This causes persistent nausea and vomiting. Over time, the remaining stomach will often stretch out until it becomes possible to eat small meals.
The stomach’s capacity for holding food is reduced so much that it is often impossible to eat. A liquid diet is often necessary in the postoperative period. Eating any more than a thimbleful will result in severe gastric distention, ballooning of the miniature stomach. This causes persistent nausea and vomiting. Over time, the remaining stomach will often stretch out until it becomes possible to eat small meals.
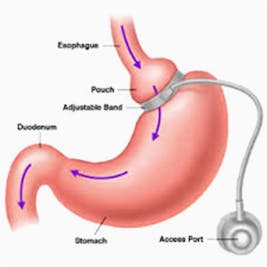
Removing large portions of healthy stomach is not ideal, so the lap band was developed. This involves the surgical implantation of a band that simply wraps around the stomach. Like cinching a tight belt, the lap band restricts food from entering the stomach and eliminates the need to cutting anything out. The lap band can be gradually tightened or loosened as needed.
In the short term, all types of bariatric surgery are effective for weight loss and diabetes. Longer-term studies show varied effectiveness. As the stomach expands, patients often resume their previous eating habits, since surgery has not taught them proper weight-loss techniques. However, my point is not to praise or condemn these surgeries. As with everything else in medicine, they do have their place. My main question is what happens to the type 2 diabetes? In virtually all cases, it simply disappears. Yes, it just goes away. The problem, it turns out, was not that the disease was not reversible, the problem was our treatment of the disease was incorrect.
—
Jason Fung
Try it
How to Reverse Type 2 Diabetes – The Quick Start Guide
Diabetes success stories
![Kenyan doctor reverses his type 2 diabetes with low carb, then pays it forward]() Kenyan doctor reverses his type 2 diabetes with low carb, then pays it forward
Kenyan doctor reverses his type 2 diabetes with low carb, then pays it forward![How Mike broke free from food addiction with a keto diet]() How Mike broke free from food addiction with a keto diet
How Mike broke free from food addiction with a keto diet![‘Keto is a way I can eat because I love the food!’]() ‘Keto is a way I can eat because I love the food!’
‘Keto is a way I can eat because I love the food!’!["I'm feeling much better at 50 than 40!"]() "I'm feeling much better at 50 than 40!"
"I'm feeling much better at 50 than 40!"![Adam 'struggled to keep weight off' until he tried keto]() Adam 'struggled to keep weight off' until he tried keto
Adam 'struggled to keep weight off' until he tried keto





Top videos about type 2 diabetes
![My low-carb story with Marc Gossange]()
![Living low carb with Chris Hannaway]()
- MEMBERS ONLY
!["I have been following the wrong advice!"]()



Top videos with Dr. Fung
![Diet Doctor Podcast #64 with Jason Fung]()
- MEMBERS ONLY
![Part 8 of Dr. Jason Fung's diabetes course]()
- MEMBERS ONLY
![The essential problem with type 2 diabetes]()


Earlier with Dr. Jason Fung
Intermittent Fasting Does Not Cause Muscle Loss
Triglycerides and Heart Disease – What’s the Connection?
Complications of Diabetes – A Disease Affecting All Organs
More with Dr. Fung
Dr. Fung has his own blog at intensivedietarymanagement.com. He is also active on Twitter.His book The Obesity Code is available on Amazon.
His new book, The Complete Guide to Fasting is also available on Amazon.