Type 2 diabetes

Type 2 diabetes is by far the most common form of diabetes (around 90% of all cases).1
The disease is getting more and more common, and there’re already an estimated 330-500 million people with type 2 diabetes worldwide.2
Most, but not all, people who are affected are overweight (especially those carrying excess abdominal fat), are middle aged or older, and may have high blood pressure, low HDL and high triglycerides.3 Although there is a growing trend of younger people, even teenagers, developing type 2 diabetes.4
For more on the background to the epidemic, how you can test if you have diabetes and how to naturally regulate your blood sugar, please read our evidence-based guide:
Diabetes – normalize your blood sugar
Here you’ll find more specific information on the cause of and treatment for type 2 diabetes.
Table of contents
- The cause of type 2 diabetes
- Treatment
- Other lifestyle modifications
- Dietary supplements
- Medications
- More education
The cause of type 2 diabetes
Type 2 diabetes results when the body can no longer handle large amounts of circulating blood sugar.5 As the blood sugar increases, the body needs to produce larger amounts of the blood sugar-lowering hormone insulin. However, over time sensitivity to insulin can decrease and the blood sugar rises out of control. At the time of diagnosis, people with type 2 diabetes often have ten times more insulin in their bodies than what’s normal.6 As a side effect all this insulin can lead to fat storage and weight gain, something that often has been going on for many years before the disease is diagnosed.7
So what’s the cause of this? This is still controversial and much debated. But there appears to be a clear correlation with the amount of sugar in the food. The more sugar people consume the more they get diabetes in the long run. According to a recent investigation this correlation is found in all countries around the world.8

Simple carbohydrates
Probably also contributing is ingestion of other rapidly-digested carbohydrates, such as white bread and pasta, because these too cause a rapid rise in blood sugar.9 Here too there are clear linkages: people who eat more simple carbohydrates are more likely to get type 2 diabetes.10
The associations between sugar, rapidly-digested carbohydrates and type 2 diabetes hold even in more rigorous studies. To give advice in favor of carbohydrate-rich food increases the risk of getting type 2 diabetes and worsens blood sugar levels in people who already have type 2 diabetes.11
Type 2 diabetes could thus very well be called sugar disease. And since starch in bread turns into glucose in the body – white flour is in fact also a form of sugar.12
Treatment of type 2 diabetes

How do we treat type 2 diabetes? Old wisdom and new science produce the same logical answer. The most important thing is to avoid eating too much blood sugar-raising food.13
Avoid eating large amounts of sugar and starch and your blood sugar will be better from the first meal on. Your high insulin levels will likely drop towards normal levels.14 Because insulin is a fat storing hormone when insulin levels drop most people gradually lose weight as well.15
If you’re lucky, especially if you haven’t had type 2 diabetes very long, this action may be all that’s needed to reverse your diabetes and become healthy.16
Try it yourself: LCHF for beginners
NOTE: If you’re being treated with insulin, insulin-releasing tablets (Sulfonylureas) or other blood sugar medications, you may need to taper off your medications if you are eating fewer carbohydrates. Please do not attempt to do this on your own. Discuss this with your doctor before changing your diet as you may be at risk for dangerously low blood sugar levels. If you do experience low sugar levels, make sure to eat something sugary right away and contact your doctor immediately.
Other lifestyle modifications
Although other lifestyle habits can help treat type 2 diabetes, eating significantly fewer carbohydrates is definitely the most important thing.17 We recommend that initially you put all of your self-discipline into changing your eating habits. It’s hardest in the beginning (first weeks and months), and likely gets easier over time.
Gradually, as your new eating habits start to flow easier you can start trying other beneficial lifestyle changes such as:
Dietary supplements
According to recent studies there is one supplement that can help many with type 2 diabetes a little: Vitamin D. Many people are deficient in Vitamin D, especially during the winter months. 18 Studies show that supplementation can improve blood sugar and insulin sensitivity somewhat in type 2 diabetes. In addition this may help with weight loss.19
Around 4 000 IU daily (100 µg) may be appropriate for most people with type 2 diabetes. However, this may depend on your baseline level, so ask your doctor for a simple blood test to see where you are and if vitamin D supplementation is right for you.
Medication
If diet changes and other lifestyle changes don’t improve blood sugar sufficiently, then you doctor may suggest stating medications. Although medications have a role, it is interesting to note that studies have shown worse outcomes with more aggressive medical therapy.20 So far, this has not been shown with lifestyle therapy. In fact, the opposite is likely true!21
1. Metformin
Metformin is the first-line treatment of choice. It’s an old and proven treatment that not only improves blood sugar, but it also aids in weight loss and potentially improves survival for those with type 2 diabetes.22
The most common side effects are stomach pain, nausea, or diarrhea. These usually subside with time, but your doctor may want to start at a low dose and titrate it up over time if needed.
A dose of two grams daily is often sufficient for a positive effect, and the maximum dose is three grams daily.
2. GLP-1 analogues or SGLT-2 Inhibitors?
When Metformin isn’t sufficient, or if you don’t tolerate it, then what to do? This is controversial today.
Often insulin injections are used. However, since overweight patients with type 2 diabetes already have pathologically high insulin levels, adding MORE insulin in this situation doesn’t make much sense. It will often cause a gradually worsening insulin resistance and obesity. Although not conclusive, it may even increase the risk of heart disease or death.23
Newer and potentially better alternatives are GLP-1 Agonists and SGLT-2 inhibitors.
GLP-1 agonists are injections that increase satiety, lower blood sugar and often lead to substantial weight loss (over 20 lbs is common). Together with Metformin, the effect on the majority of patients is very positive for both blood sugar and weight.
SGLT-2 inhibitors stimulate the kidneys to excrete excess glucose, thus lowering the blood glucose level without increasing circulating insulin. In fact, insulin levels tend to go down. Trials have shown reduced cardiovascular events in people with diabetes taking SGLT-2 inhibitors.24. However, they unfortunately can increase the risk of a life threatening condition called euglycemic ketoacidosis, especially in those eating ketogenic diets.25 Although this is very rare, we do not recommend SGLT-2 inhibitors for those who are eating low-carb.
Our hope, of course, is for you to take control of diabetes with low-carb nutrition so that you do not need any of these medications. Make sure you discuss your progress with your physician to see if you require medication or not.
Insulin![bloodsugarmeasuring]()

Sometimes pills are not enough to control dangerous blood sugar levels and your doctor may recommend insulin injections. These are not without their concerns as they are expensive, may lead to weight gain, and they can also exacerbate the underlying disease by worsening hyperinsulinemia and insulin resistance.26
Fortunately, studies show that patients can quickly and dramatically reduce their need for insulin with low-carb diets.27 Therefore, if you are on insulin, please talk to your doctor before going on a low-carb diet as you will likely need to reduce your dose to prevent dangerously low blood sugar levels (hypoglycemia). Learn more in our guide Starting low carb or keto with diabetes medications.28
More education
Can you reverse type 2 diabetes?29
Can you reverse diabetes in only six months? Without medications or surgery? Now science says you can. Two different nonrandomized trials demonstrated that low carbs diets are effective at normalizing blood sugar while also reducing the need for medications.30
No expensive injections. No surgery. Just low-carb nutrition. That’s powerful.
Read more in our guide on reversing diabetes.
You can also read more blog posts about people with type 2 diabetes that have tried a low-carbohydrate diet [1 2] and inspirational stories from people who have taken control of their diabetes with low-carb nutrition.31
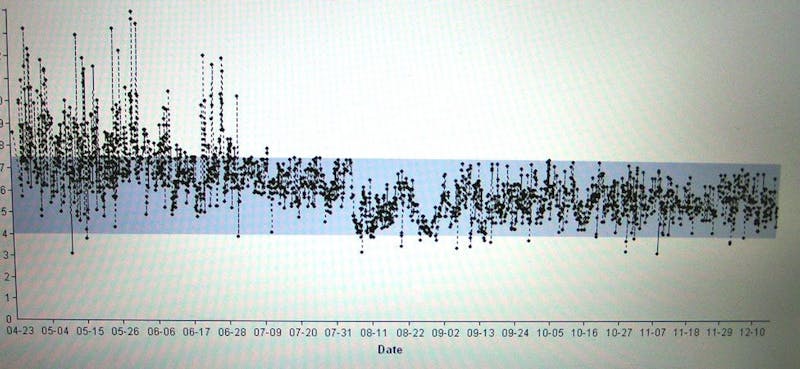
For example, pictured below is a large number of blood glucose readings in a person with type 2 diabetes in the first six months on an LCHF diet. The blue area corresponds to optimal blood glucose levels. Note that not one single elevated number was recorded after a few months! And then after just three days she was even able to stop daily 70E insulin injections. She also lost 68 lbs in the first year.32
Studies on an LCHF diet for type 2 diabetes
Self monitoring
Monitoring your blood sugar yourself seems to have a small positive effect, even for people with diabetes not taking insulin.33
Of course, how great the effect will be depends entirely on whether the monitoring leads to an improved lifestyle. Just checking your blood sugar and writing down the number in a book will of course not make you any healthier at all. Instead, monitoring of blood sugar can be used to help improve diet and exercise and adjust medications as needed.
We can do better
High blood sugar produces a risk for severe complications in the long run. It degrades the body’s small blood vessels, increasing the risk for heart attack, blindness, amputations and more.34
Millions of patients have suffered these complications while the medical establishment tries to “manage” the disease. Even popular press such as the New York Times promotes the concept that type 2 diabetes is a chronic progressive disease that we are failing to treat. We disagree and so should you.
It may be true that a conventional low-fat diet (today’s dietary guidelines) and medications don’t cure diabetes. But fortunately, a better treatment exists, and it’s obvious and logical when you understand.
We promote the science and practical aspects of using low carb to treat type 2 diabetes so the millions of people at risk can take charge of their own health and avoid suffering preventable complications.
Please keep reading and learn more in our guide How to reverse your diabetes
Presentation

A presentation on diabetes and a low-carbohydrate diet by Mary C. Vernon, an American physician, since long specializing on the subject.
Related links
Type 2 diabetes - the evidence
This guide is written by Dr. Andreas Eenfeldt, MD and was last updated on June 17, 2022. It was medically reviewed by Dr. Bret Scher, MD on April 3, 2020.
The guide contains scientific references. You can find these in the notes throughout the text, and click the links to read the peer-reviewed scientific papers. When appropriate we include a grading of the strength of the evidence, with a link to our policy on this. Our evidence-based guides are updated at least once per year to reflect and reference the latest science on the topic.
All our evidence-based health guides are written or reviewed by medical doctors who are experts on the topic. To stay unbiased we show no ads, sell no physical products, and take no money from the industry. We're fully funded by the people, via an optional membership. Most information at Diet Doctor is free forever.
Read more about our policies and work with evidence-based guides, nutritional controversies, our editorial team, and our medical review board.
Should you find any inaccuracy in this guide, please email andreas@dietdoctor.com.
Type 1, usually diagnosed in kids, makes up the rest. However, there are two other forms of diabetes. Latent Autoimmune Diabetes of Adults LADA is a form that has been described as “halfway between type 1 and type 2.” As with type 1 you have antibodies that attack the insulin producing beta cells. LADA usually debuts later in life then type 1 and develops more slowly. Maturity onset diabetes of the young, MODY, is a rarer form that is caused by a genetic abnormality and also mimics type 1 but is diagnosed in adults.
BMJ 2018: Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: population based study [observational study, weak evidence]
↩Diabetes 2018: Global prevalence of type 2 diabetes over the next ten years (2018-2028) [review of observational studies; weak evidence]
Medicine 2014: Epidemiology of diabetes [review of observational studies; weak evidence] ↩
BMJ 2018: Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: population based study [observational study; weak evidence] ↩
World Journal of Diabetes 2013 Type 2 diabetes mellitus in children and adolescents. [overview article; ungraded] ↩
Diabetes Care 1992: Pathogenesis of NIDDM. A balanced overview. [overview article; ungraded] ↩
American Journal of Clinical Nutrition 1992: Surgical treatment of obesity and its effect on diabetes: 10-y follow-up. [observational study, weak evidence]
Diabetes Care 2012: Diabetes: Have we got it all wrong? [overview article; ungraded] ↩
Although this is still controversial for some, the following review article summarizes insulin’s role in obesity, and the subsequent reference shows how inhibiting insulin secretion aids in weight loss. Taken together, it seems very likely that insulin has a direct action of increasing obesity.
Journal of Endocrinology 2017: A causal role for hyperinsulinemia in obesity. [overview article; ungraded]International Journal of Obesity Related Metabolic Disorders 2003: Suppression of insulin secretion is associated with weight loss and altered macronutrient intake and preference in a subset of obese adults [observational study, weak evidence] ↩
PLoS One 2013: The relationship of sugar to population-level diabetes prevalence: an econometric analysis of repeated cross-sectional data. [observational study, weak evidence]
BMC Public Health 2014: Per capita sugar consumption and prevalence of diabetes mellitus–global and regional associations. [observational study, weak evidence]
↩PLoS Biology 2018: Glucotypes reveal new patterns of glucose dysregulation. [nonrandomized study, weak evidence] ↩
American Journal of Clinical Nutrition 2008: Glycemic index, glycemic load, and chronic disease risk–a meta-analysis of observational studies. [observational study, weak evidence] ↩
Nutrients 2018: The effect of dietary glycaemic index on glycaemia in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. [strong evidence]
PLoS One 2014: A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes. [randomized trial; moderate evidence]
↩European Journal of Clinical Nutrition 1992: Classification and measurement of nutritionally important starch fractions. [mechanistic study article; ungraded]
The following RCT showed that all types of bread, including sprouted and multi-grain, caused an elevation in blood sugar and serum insulin levels.
Journal of Nutrition and Metabolism 2012: The acute impact of ingestion of sourdough and whole-grain breads on blood glucose, insulin, and incretins in overweight and obese men. [randomized trial; moderate evidence]
↩Diabetes Care 2019: Nutrition therapy for adults with diabetes or prediabetes: a consensus report [overview article; ungraded] ↩
Annals of Internal Medicine 2005: Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. [observational study, weak evidence] ↩
Nutrition and Diabetes 2017: Enhanced insulin sensitivity in successful, long-term weight loss maintainers compared with matched controls with no weight loss history. [nonrandomized study, weak evidence] ↩
Some disagree with the use of the word “reverse” when it comes to type 2 diabetes. The concern is that it may imply the disease is completely gone, never to return. At Diet Doctor, we use the term “reverse” to indicate that the diagnosis of diabetes is no longer present at that moment. However, we acknowledge that the diagnosis of diabetes will likely return if a patient goes back to their prior high-carb eating habits. Therefore, “reverse” does not imply a cure. Instead, it identifies a successful intervention that, if maintained, will likely keep the disease at bay.
The following study showed a ketogenic diet was effective at reversing diabetes or reducing medications in the majority of subjects.
Frontiers in Endocrinology 2019: Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of type 2 diabetes: A 2-year non-randomized clinical trial [weak evidence]
↩This is based on consistent clinical experience of low-carb practitioners. [weak evidence] ↩
Nutrition Research 2011: Prevalence and correlates of vitamin D deficiency in US adults. [observational study, weak evidence] ↩
Although there is conflicting data on the subject, these studies suggest a potential benefit from vitamin D supplementation
Nutrition Journal 2012: A 12-week double-blind randomized clinical trial of vitamin D3 supplementation on body fat mass in healthy overweight and obese women [moderate evidence]
Journal of the American College of Nutrition 2016: The effect of vitamin D supplementation on glycemic control and lipid profile in patients with type 2 diabetes mellitus. [noncontrolled study, weak evidence] ↩
NEJM 2008: Effects of intensive glucose lowering in type 2 diabetes. [randomized trial; moderate evidence]
The Lancet 2010: Survival as a function of HbA1c in people with type 2 diabetes: a retrospective cohort study [observational study; weak evidence]
However, more recent trials of the drug class SGLT2 inhibitors do show an improvement in cardiovascular outcomes and risk of death. One hypothesis is that these drugs lower insulin levels whereas older drugs increased insulin levels.
NEJM 2015: Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. [randomized trial; moderate evidence]
Cardiovascular Ultrasound 2019: Effect of sodium glucose cotransporter 2 inhibitors on cardiac function and cardiovascular outcome: a systematic review [overview article; ungraded]
↩The studies that show no improvement with more intensive medications included insulin and medications that increased insulin. Newer drugs, like the SGLT2 inhibitors, can lower insulin and have been shown to improve risk of heart disease or overall mortality. Since lifestyle interventions, like low-carb diets and exercise, also lower both glucose and insulin, one could assume they would likewise show beneficial results although this has yet to be studied in adequately designed long-term trials.
The following trial, called the LOOK AHEAD trial, is frequently cited as evidence that lifestyle interventions do not improve clinical outcomes in patients with diabetes. However, the intervention was general calorie reduction and did not address carbohydrate intake.
NEJM 2013: Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. [randomized trial; moderate evidence] ↩
JNCI Cancer Spectrum 2017: The effect of metformin on mortality among cancer patients with diabetes: A systematic review and meta-analysis [review of observational studies, weak evidence] ↩
Experimental and Therapeutic Medicine 2016: Association between insulin dosage and insulin usage time, and coronary artery lesions in patients with type 2 diabetes and coronary heart disease [observational study, weak evidence]
European Heart Journal 2007: The impact of glucose lowering treatment on long-term prognosis in patients with type 2 diabetes and myocardial infarction: a report from the DIGAMI 2 trial [observational study, weak evidence]
Diabetologia 2009: The influence of glucose-lowering therapies on cancer risk in type 2 diabetes. [observational study, weak evidence]
NEJM 2008: Effects of intensive glucose lowering in type 2 diabetes. [randomized trial; moderate evidence]
↩NEJM 2015: Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. [randomized trial; moderate evidence] ↩
Diabetes Care 2015: Euglycemic diabetic ketoacidosis: A predictable, detectable, and preventable safety concern with SGLT2 inhibitors[case reports; very weak evidence] ↩
Journal of Endocrinology and Metabolism 1997: Effect of obesity on the response to insulin therapy in noninsulin-dependent diabetes mellitus. [nonrandomized study, weak evidence]
Nature Medicine 2017: Insulin action and resistance in obesity and type 2 diabetes. [overview article; ungraded]
↩Nutrition & Diabetes 2017: Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes [moderate evidence]
Diabetes Therapy 2018: Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: an open-label, non-randomized, controlled study [weak evidence] ↩
With insulin-treated diabetes it’s important to monitor your blood sugar closely in the beginning when starting an LCHF diet! A diet including few carbohydrates usually causes a greatly reduced need for insulin. It’s then important to adjust (lower) the doses sufficiently to avoid blood sugar droping too low. This should always be done with support of your physician or diabetes nurse. ↩
Some disagree with the use of the word “reverse” when it comes to type 2 diabetes. The concern is that it may imply the disease is completely gone, never to return. At Diet Doctor, we use the term “reverse” to indicate that the diagnosis of diabetes is no longer present at that moment. However, we acknowledge that the diagnosis of diabetes will likely return if a patient goes back to their prior high-carb eating habits. Therefore, “reverse” does not imply a cure. Instead, it identifies a successful intervention that, if maintained, will likely keep the disease at bay. ↩
Diabetes Therapy 2018: Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: an open-label, non-randomized, controlled study [weak evidence]
The longest published study yet on low carb for type 2 diabetes, is a non-randomized intervention trial of a 20% carbohydrate diet for people with obesity and type 2 diabetes. They published a 44-month follow-up showing continued good results on A1c, weight, and reduction of diabetes medications:
Nutrition & Metabolism 2008: Low-carbohydrate diet in type 2 diabetes: stable improvement of bodyweight and glycemic control during 44 months follow-up [weak evidence] ↩
BMJ 2012: Meta-analysis of individual patient data in randomised trials of self monitoring of blood glucose in people with non-insulin treated type 2 diabetes. [systematic review of randomized trials; strong evidence] ↩
Clinical Diabetes 2011: Microvascular and macrovascular complications of diabetes [overview article; ungraded] ↩