
Understanding absolute and relative risk
With chronic diseases, one of the most deceptive “sleights of hand” with numbers is the use of relative risk to report the size of an effect found in a study. Relative risk confuses unsuspecting readers; it can make even a tiny effect seem very large.
Let’s take a look at the differences between absolute risk and relative risk.
Absolute risk is the chance, or probability, that a specific health event will happen to you (or to anyone in a similar group of people).
Relative risk, on the other hand, is the chance, or probability, that people in one group will experience a health event compared to people in another group.
You might ask, “Why does this matter?” Well, the two numbers — in exactly the same treatment scenario — can appear drastically different, with absolute risk being a very small number and relative risk seeming to be very large. This can distort perceptions about how successful and worthwhile a specific medical treatment may be for you personally.
For example, say in a group of 100 people, there is a risk that two people will have a heart attack. If you are in that group, your absolute risk of a heart attack is 2%. Now, let’s say researchers conduct a study of a drug treatment for this condition. One group of 100 people gets a placebo (the control group), and another group of 100 people gets the drug — which could have significant side effects.
The study finds that while the control group had the expected two heart attacks, the treatment group had just one. Also, in the treatment group, 15 people experienced significant side effects. The absolute risk decreased by only 1% but the relative risk decreased by 50%! Your doctor might tell you “people who took this drug had a 50% better outcome.” But your risk is really reduced by just 1% if you take the drug and there will be a 15% risk of experiencing the side effects.
A real-world example
The classic example of this type of finding is with statin drugs for primary prevention of cardiovascular events. The JUPITER trial was a well-controlled, randomized clinical trial that took 17,802 healthy subjects 1 and treated half of them with a statin (20 mg of rosuvastatin or Crestor) and half with a placebo.
Here are the results after about two years:
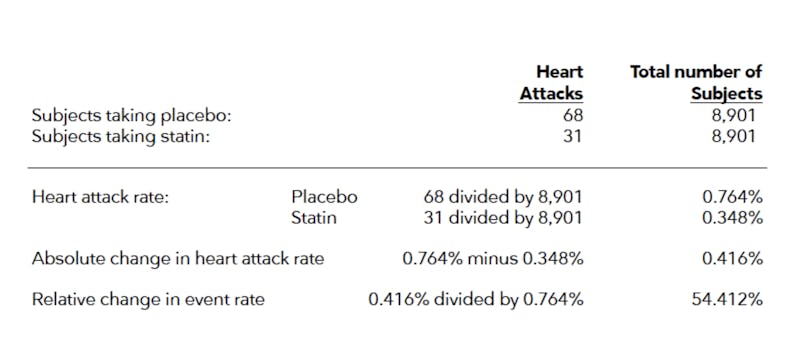
Absolute risk
We could truthfully say that subjects taking a statin reduced their risk of a heart attack from 0.76% to 0.35%, or about 0.42%. Not very impressive. Would you commit to taking a pill every day for the rest of your life to reduce your risk of a heart attack by 0.42% over two years? Maybe… but if it also meant a significant and much larger risk of side effects, you perhaps would not.
Relative risk
Conversely, we could truthfully report that subjects taking a statin reduced their rate of heart attacks by 54% relative to those taking placebo. That sounds very impressive, so if you are looking for a headline to sell drugs, this would likely be the way you would present the study results.
What’s the bottom line?
Relative risk sometimes makes tiny changes in absolute risk seem very big. It can make patients believe that an intervention dramatically reduces their risk of harm, when the protection, in absolute terms, is quite small.



Subjects had no history of heart disease and LDL cholesterol levels below 130mg/dL. However, subjects also had elevated C-reactive protein levels, which is a sign of systemic inflammation ↩