
Aiming to understand the dawn effect
By Dr. Bret Scher, MD, medical review by Dr. William Yancy, MD
Evidence based
Have you noticed that your blood sugar rises first thing in the morning? Is your morning glucose reading sometimes your highest at that time of the day? If so, you are not alone.
As low-carb diets and intermittent fasting become more popular, more people experience the so-called “dawn effect” or “dawn phenomenon.” But why does it happen? And, more importantly, is it anything of concern?
This guide will walk you through the science behind the dawn effect, focusing on what we know and what we don’t know as it applies to low-carb nutrition.
What is the dawn effect?
The dawn effect refers to an unexpected increase in fasting blood sugar, usually upon waking. Doctors first noted it in patients with type 1 diabetes in the 1980s. They defined the dawn effect as rising blood sugar without the usual compensatory rise in insulin.1
As morning approaches, the body naturally increases glucose production. However, the insulin the patients took the night before was insufficient to control the glucose rise. The mismatch led to an increase in blood glucose.
Researchers determined that the early morning glucose rise was caused by an increase in the so-called “counterregulatory hormones” cortisol, epinephrine, and norepinephrine.2 They are called counterregulatory hormones primarily because they “counter” the effects of insulin.
These counterregulatory hormones stimulate the liver to secrete glucose into the body. If an individual has a normal insulin response, their insulin level rises to keep their blood glucose level stable.
For individuals experiencing the dawn effect, the extra glucose circulates until it is taken up by the cells and used for energy. You can think of this as the body preparing itself for the increased energy demands needed to wake up and ensure enough glucose is ready for use as a person becomes active each morning.
Studies in people without diabetes show the body increases insulin secretion between 4 am and 8 am. This extra boost of insulin acts to stabilize the increase blood glucose levels from the counterregulatory hormones.
3Therefore, for decades, the dawn effect was assumed to be a problem only for those with type 1 or type 2 diabetes. But now, that assumption may be changing.
Implications
For people with diabetes, a prominent dawn effect signifies an inability to control morning blood sugar and may have long-term health consequences.
One study showed the dawn effect is associated with a 0.4% (4 mmol/mol) increase in hemoglobin A1c (HbA1c) levels, which roughly reflect the 3-month average of blood sugar levels.4
Since higher HbA1c levels correlate with a higher risk of complications, the dawn effect likely has harmful health consequences for those with diabetes. The current recommendation is to aggressively treat the dawn effect with medications to improve overall glucose control.5
But what about people who don’t have diabetes? Or, what if they follow a low-carb diet and preferentially burn fat for fuel instead of glucose? Would the dawn effect have the same implications? We’ll explore that next.
The dawn effect in fat burners
First comes the bad news. We are not aware of any scientific studies that look at the dawn effect in individuals who follow a very low-carb diet.
However, based on clinical experience, the dawn effect is relatively common among those following a strict low-carb diet.6
Remember the physiology. As you get closer to waking, your body secretes counterregulatory hormones, which increase the liver’s glucose output. But if the blood glucose rises, that implies the compensatory rise in insulin is not present. Why would this be?
Again, there isn’t any concrete evidence to explain why blood sugar rises, but there are theories.
One theory is that the pancreas doesn’t need to respond quickly to elevated blood sugar since it rarely happens on a very low-carb diet. In essence, the feedback loop rebalances.7
Another theory focuses on muscle cells. Under glucose-burning conditions, muscle cells are the prime driver of glucose uptake, taking glucose out of the blood to use it for energy.
However, when your cells instead primarily burn fat for fuel, as they do when dietary carbohydrate is dramatically reduced, the muscle cells don’t need glucose. The brain, on the other hand, still needs some glucose. Muscle cells become “resistant” to glucose so that the brain can be “first in line” for available glucose.
Many call this physiologic process “adaptive glucose sparing” or “physiologic insulin resistance.” The idea is that the lack of glucose uptake happens for a beneficial reason, not a harmful reason, as it does in diabetes. Again, this is a theory, but it is a theory that makes sense in terms of how the body works.
Some believe insulin resistance provided an evolutionary advantage to our hunter-gatherer ancestors, allowing their brains to use glucose while encouraging their muscles to run on fat.8
One fundamental difference between potentially harmful and likely benign elevated glucose could be the presence or absence of elevated insulin levels. Elevated glucose in a setting of insulin resistance with elevated insulin levels likely has a different biological outcome than the same glucose in a setting of insulin sensitivity and low insulin levels.
While that does not mean for certain that the two situations have different outcomes, the different effects in the body suggest they might.
Is the dawn effect always harmful?
While research suggests the dawn effect is potentially harmful to individuals with type 2 diabetes, can we say the same for those without diabetes?9
Without research to guide us, we have to use our best reasoning skills to reach a hypothesis.
Blood glucose appears to exert harmful effects in two ways. One is when glucose is chronically elevated, and the other is when blood glucose levels have large increases or “spikes,” known as the glucose variability.10
Studies show both mechanisms accelerate vascular and endothelial dysfunction11
We could conclude that if neither of these concerns is present — there is no chronic elevation, and the rise or spike is relatively small — there should not be concerning vascular or other health consequences.12
How do we measure or define “chronic elevation?” It’s usually measured by HbA1c. The higher that is, the higher the average blood sugar. It isn’t perfect, but it’s a useful marker that approximates chronic blood sugar elevation.
However, HbA1c may not account for shorter, more intense blood sugar elevations, also referred to as glycemic variability.
A post-meal glucose increase up to 140 mg/dL (7.8 mmol/L) is considered normal.13
Therefore, we may infer that a dawn effect up to 140 mg/dL (7.8 mmol/L) should not be a cause of concern.
This may be especially true if morning blood sugar levels are the highest levels of the day, and post-meal levels after low-carb meals are significantly lower. Again, there are no data on this, so it is a hypothesis. But it makes sense.
Based on this theory, if HbA1c is in the normal range or improving, dawn blood glucose levels do not exceed 140 mg/dL (7.8mmol/L), and post-meal elevations are lower than 140 mg/dL (7.8mmol/L), then it seems reasonable that the dawn effect is not a clinical concern.14
However, if these criteria are not met, the morning elevation may be adding to an ongoing problem and accelerating vascular damage.
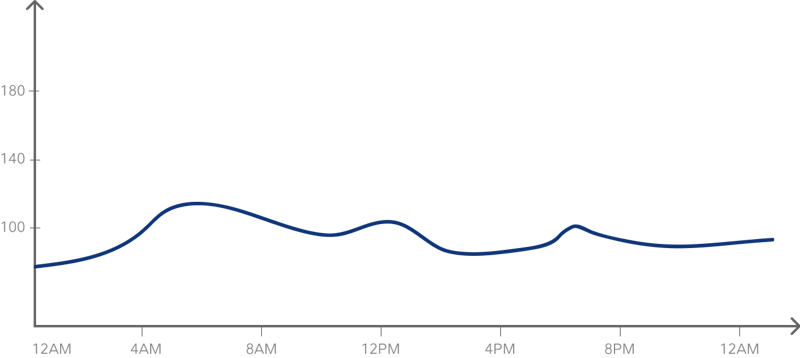
As an example, here is a representation of a continuous glucose monitor (CGM) graph that would suggest more of a chance the dawn effect will not have negative health consequences.. Notice the peak glucose level is 120 mg/dL (6.7 mmol/L), and it is the highest level of the day, with post-meal peaks staying below 110 mg/dL (6.1 mmol/L) and returning to baseline within an hour.
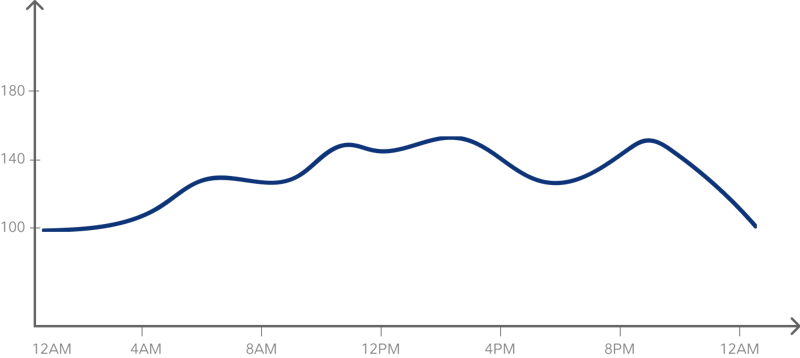
On the other hand, this graph suggests that the dawn effect is part of a larger problem. The blood sugar starts high, with a peak of 130 mg/dL (7.2 mmol/L), and it never gets back to baseline before rising again to well above 140 mg/dL (7.8 mmol/L) after meals.
These two graphs differ in the following ways:
- The degree of blood sugar elevation
- the chronic nature of blood sugar elevation
- the likely underlying mechanisms for the blood sugar rise
Can you decrease the dawn effect?
For some individuals, the dawn effect may not be a concern. But if you feel it could contribute negatively to your health, what can you do to lessen it?15
- Exercise may help. Doing some form of physical exertion after dinner and first thing upon waking may reduce the degree and duration of the glucose increase.16
- Also, eating early in the morning can help reduce the dawn effect. This advice may seem paradoxical. Wouldn’t eating raise blood sugar? Not in this case.
Remember, the dawn effect is caused by lower than usual insulin secretion in the morning to ensure adequate glucose levels. If you eat food, that will signal to your body that you have sufficient energy, and your insulin may respond appropriately. The result is enough insulin to help bring down your glucose level17
- Some people recommend eating a low-carb, high-fat or high-protein snack before bed to minimize the dawn effect. For those trying to benefit from intermittent fasting, this is not a great option. But it may be a better choice than starting a medication. Each individual should determine if this recommendation is right for them.
Testing your blood glucose in the morning can tell you if this strategy helps.- Don’t forget the importance of sleep! A poor night of sleep can increase cortisol production, leading to a more significant dawn effect.18
- Lastly, some may consider the use of medications. Taking insulin in the evening tends to be more effective than oral diabetes medications at reducing the degree and duration of glucose elevation.19
All medications, especially insulin, have potential side effects, including the risk of dangerously low blood sugar. You should discuss possible medication changes with your healthcare provider and ask for a thorough risk-benefit analysis.
Summary
We know a great deal about the dawn effect as it relates to diabetes and an increased risk of potential complications. However, we know much less about the dawn effect in people following a low-carb diet whose muscles primarily burn fat rather than glucose for fuel.
For many, the mild morning blood sugar rise is likely an adaptation that is not a health concern. But until we have more scientific evidence, it is prudent to investigate morning blood sugar elevations with a healthcare professional and, if concerning, consider available tools to address them.
/ Dr. Bret Scher, MD



Understanding the dawn effect — what we know and don’t know - the evidence
This guide is written by Dr. Bret Scher, MD and was last updated on June 19, 2025. It was medically reviewed by Dr. William Yancy, MD on November 23, 2020.
The guide contains scientific references. You can find these in the notes throughout the text, and click the links to read the peer-reviewed scientific papers. When appropriate we include a grading of the strength of the evidence, with a link to our policy on this. Our evidence-based guides are updated at least once per year to reflect and reference the latest science on the topic.
All our evidence-based health guides are written or reviewed by medical doctors who are experts on the topic. To stay unbiased we show no ads, sell no physical products, and take no money from the industry. We're fully funded by the people, via an optional membership. Most information at Diet Doctor is free forever.
Read more about our policies and work with evidence-based guides, nutritional controversies, our editorial team, and our medical review board.
Should you find any inaccuracy in this guide, please email andreas@dietdoctor.com.
Diabetes Care 1981 The dawn phenomenon, an early morning glucose rise: implications for diabetic intraday blood glucose variation [small observational study, weak evidence] ↩
Diabetes 1996: Evidence for a circadian rhythm of insulin sensitivity in patients with NIDDM caused by cyclic changes in hepatic glucose production [nonrandomized study, weak evidence] ↩
Diabetes Care 1984: Fasting early morning rise in peripheral insulin: evidence of the dawn phenomenon in nondiabetes
[nonrandomized study, weak evidence] ↩Diabetes Care 2013: Magnitude of the dawn phenomenon and its impact on the overall glucose exposure in type 2 diabetes: is this of concern? [nonrandomized study, weak evidence] ↩
Diabetes Care 2013: Thirty years of research on the dawn phenomenon: lessons to optimize blood glucose control in diabetes [overview article; ungraded] ↩
This is based on consistent clinical experience of low-carb practitioners. [weak evidence] ↩
Some hypothesize that the brain can change the set point at which the body needs to respond to glucose elevations. While the data mostly pertains to animals, it makes an intriguing potential explanation for the lack of insulin response in the dawn effect.
Diabetologia 2020: Brain control of blood glucose levels: implications for the pathogenesis of type 2 diabetes
[overview article; ungraded] ↩Clinical Nutrition 2012: The evolutionary benefit of insulin resistance [overview article; ungraded] ↩
Diabetes care 2013 Magnitude of the dawn phenomenon and its impact on the overall glucose exposure in type 2 diabetes: is this of concern? [nonrandomized study, weak evidence] ↩
The DCCT trial showed chronically elevated blood sugar was linked to worse clinical outcomes, and intensive management of blood sugar reduced death disability.
NEJM 2005: Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes
[randomized trial; moderate evidence]The following is a review about what glycemic variation is and how to measure it.
Diabetes Metabolism Journal 2015: Glycemic Variability: How do we measure it and why is it important?
[overview article; ungraded]The following study suggests glycemic variability is a stronger predictor of poor outcomes compared to fasting blood sugar
Journal of Clinical Endocrinology and MEtabolism 2006: Postprandial blood glucose is a stronger predictor of cardiovascular events than fasting blood glucose in type 2 diabetes mellitus, particularly in women: lessons from the San Luigi Gonzaga Diabetes Study [nonrandomized study, weak evidence]The following study showed the association between glucose variability and increased cardiovascular risk was much greater with type 2 compared to type 1 diabetes
Diabetes, Obesity, and Metabolism 2010: Glycaemic variability and complications in patients with diabetes mellitus: evidence from a systematic review of the literature [meta analysis of randomized and nonrandomized studies, weak evidence] ↩
Diabetes Research and Clinical Practice 2008: Glucose “peak” and glucose “spike”: Impact on endothelial function and oxidative stress [nonrandomized study, weak evidence]
International Journal of Vascular Medicine 2012 Hyperglycemia and endothelial dysfunction in atherosclerosis: lessons from type 1 diabetes
[randomized trial; moderate evidence]Circulation 1996: Chronic hyperglycemia impairs endothelial function and insulin sensitivity via different mechanisms in insulin-dependent diabetes mellitus
↩
[nonrandomized study, weak evidence]This is based on a hypothesis derived from mechanistic and outcome studies — but is not based on research data. ↩
Diabetes Care 2001: Postprandial blood glucose [overview article; ungraded] ↩
The definition of normal postprandial glucose is based on studies showing people who are more likely to progress to diabetes or prediabetes. Many clinicians believe “optimal” glucose levels are even lower, closer to 120mg/dl (6.7 mmol/L). This is based on clinical experience of low-carb practitioners. [weak evidence] ↩
The following suggestions are based on recommendations from expert opinion, clinical experience, and anecdotal reports. No studies are investigating specific interventions aside from medications. ↩
This is likely especially true if the carbohydrate content of the food is low and therefore does not raise the blood glucose much further. ↩
International Journal of Endocrinology 2017 Poor sleep quality is associated with dawn phenomenon and impaired circadian clock gene expression in subjects with type 2 diabetes mellitus [nonrandomized study, weak evidence] ↩
Diabetes Care 2013: Thirty years of research on the dawn phenomenon: lessons to optimize blood glucose control in diabetes [overview article; ungraded] ↩