Low-carb studies broken down by protein content
For the following analysis, we included 29 randomized, controlled trials (RCTs), all lasting at least three months. All of these trials measure weight loss and glycemic control for a low-carb diet compared to a control diet; they also specify the amount of protein eaten or the amount recommended. We selected these trials by reviewing all published meta-analyses of RCTs for low-carb diets.
Summary
- No trials showed low fat was better for weight loss or glycemic control.
- Seven trials kept protein equal in the two diets being compared:
- Four showed low carb worked better than control. However, one didn’t specify what participants ate, only what they were told to eat, so it is unclear if they complied or not. Another kept protein very low at only 64 grams per day.
- Three showed no difference between low carb and control.
- Nine trials showed lower carb AND higher protein resulted in similar benefits compared to the control diet.
- Thirteen trials showed lower carb AND higher protein was better than the control diet.
In conclusion, most RCTs showing low-carb diets are better than control diets (often a low-fat, calorie restricted diet) for weight loss and glycemic control also increased protein intake when carbs were reduced. Therefore, we can’t be sure if the beneficial effect was due to the lower carbs, higher protein, or both.
Similar protein intake in low-carb and comparison group
The following seven trials reported similar protein intake between the two groups with three studies reporting similar outcomes, and four reporting better outcomes in the low-carb group.
Similar protein, better outcomes in low-carb group: 4 studies
Saslow et al. (2017) compared a keto diet (20 to 50 grams of carbs per day) to the American Diabetes Association’s (ADA) “Create Your Plate” diet. The low-carb group was allowed to eat as much as they wanted as long as carbs were limited. The low-carb group ate 81 grams of protein per day and the low-fat group ate 74 grams. The small difference was not statistically significant.
The low-carb diet was better at lowering hemoglobin A1c (HbA1c) (-0.8% vs -0.3%), with 55% of participants getting below 6.5% (48 mmol/mol) compared to 0% in the low-fat group. Also, the low-carb group lost more weight on average — 28 pounds (12.7 kilos) vs. 6.6 pounds (3 kilos) — compared to the low-fat group.
Journal of Medical Internet Research: An online intervention comparing a very low-carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: a randomized controlled trial [randomized trial; moderate evidence]
Sato et al. (2017) compared calorie restriction vs “low carb.” The calorie restriction group ate 1,605 calories with 63 grams of protein and 198 grams of carbs. The “low-carb” group ate 1,372 calories with 64 grams of protein and 149 grams of carbs. (This was not a true low-carb diet.) The “low-carb” diet was better at reducing HbA1c (-0.65% vs 0%), and better at producing weight loss but not by much (-1.6 kilos vs -0.6 kilos).
Note that protein intake was the same between the control and intervention groups, but at a very low level of only 63-64 grams per day or 15% and 18% of total calories, respectively. Despite the similar protein intake, the low-carb group spontaneously reduced calorie intake by an average of 406 kcal/day, while the calorie-restriction group showed a negligible reduction in intake over the course of the study.1
Clinical Nutrition 2017: A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic control [randomized trial; moderate evidence]
Elhayany et al. (2010) compared the 2003 ADA diet with 45% carbs to a Mediterranean diet with the same amount of carbohydrate and a “low-carb” Mediterranean diet with 42% carbs. (The listed percentages represent the measured carb intake of participants, not the recommended carb intake.) The study protocol recommended 20% protein for all diets but no actual measurement was reported. Despite the minimal differences in carb intake, the low-carb Mediterranean group had a greater reduction in HbA1c than both the ADA and regular Mediterranean diets (-2% vs -1.6% and -1.8%, respectively). The low-carb group also showed greater average weight loss that did not reach statistical significance.
Diabetes, Obesity, and Metabolism 2010: A low carbohydrate Mediterranean diet improves cardiovascular risk factors and diabetes control among overweight patients with type 2 diabetes mellitus: a 1-year prospective randomized intervention study [randomized trial; moderate evidence]
Wang et al. (2018) compared a diet with 39% carbs and 19% protein to a diet with 56% carbs and 18% protein. The lower-carb group showed slightly better HbA1c reduction. Although the low-carb group lost weight compared to baseline, there was no significant difference in weight loss between groups.
Nutrients 2018: The effect of low-carbohydrate diet on glycemic control in patients with type 2 diabetes mellitus [randomized trial; moderate evidence]
Similar protein, no significant differences between groups: 3 studies
McLaughlin et al. (2007) compared a diet in which subjects consumed 52% carbs and 18% protein to one where they consumed 43% carbs and 19% protein. There were no between-group differences in weight, glucose, insulin, or triglycerides.2
Diabetes Care 2008: Clinical efficacy of two hypocaloric diets that vary in overweight patients with type 2 diabetes: comparison of moderate fat versus carbohydrate reductions [randomized trial; moderate evidence]
Wolever et al. (2008) compared three diets, all with 20% protein and either 47%, 52% or 39% carbs. There were no between-group differences in weight or HbA1c.3
American Journal of Clinical Nutrition 2008: The Canadian Trial of Carbohydrates in Diabetes (CCD), a 1-y controlled trial of low-glycemic-index dietary carbohydrate in type 2 diabetes: no effect on glycated hemoglobin but reduction in C-reactive protein [randomized trial; moderate evidence]
Krebs et al. (2012) compared a 46% carb and 21% protein diet to a 48% carb and 20% protein diet. There were no outcome differences.4
Diabetologia 2012: The Diabetes Excess Weight Loss (DEWL) Trial: a randomised controlled trial of high-protein versus high-carbohydrate diets over 2 years in type 2 diabetes [randomized trial; moderate evidence]
Increased protein intake in low-carb group
To sum up the research findings below, the first nine studies did not show a significant difference in weight loss or blood sugar between the subjects on different diets. The next 13 reported a benefit in the low-carb group.
The reason for grouping these 22 studies together is to show that the majority of the “low-carb diet” studies are also studies that increase protein, either in absolute terms or as a percentage of calories.
Increased protein with low-carb, no significant differences between groups: 9 studies
A number of these studies showed very little difference in carb intake between the groups, and some were “calorie matched.” These aspects can make it harder to show that one diet is better than the other.
Goldstein et al. (2011) compared an Atkins-style diet with 102 grams of protein to an ADA diet with 90 grams of protein. At 12 months, there were no differences in weight loss or HbA1c. Almost 50% of participants dropped out of the trial.5
The European e-Journal of Clinical Nutrition and Metabolism 2011: The effect of a low carbohydrate energy-unrestricted diet on weight loss in obese type 2 diabetes patients – A randomized controlled trial [randomized trial; moderate evidence]
Guldbrand et al. (2012) compared a diet with 20% protein and 47% carbs to a low-carb diet with 24% protein and 31% carbs. The low-carb group had better HbA1c at 6 months but not 24 months. There was no difference in weight loss.6
Diabetologia 2012: In type 2 diabetes, randomisation to advice to follow a low-carbohydrate diet transiently improves glycaemic control compared with advice to follow a low-fat diet producing a similar weight loss [randomized trial; moderate evidence]
Tay et al. (2018) compared a 25% protein and 19% carb diet to an 18% protein and 48% carb, energy-matched diet. The 2-year results report similar weight loss and HbA1c reductions.
Diabetes Obesity and Metabolism 2018: Effects of an energy-restricted low-carbohydrate, high unsaturated fat/low saturated fat diet versus a high-carbohydrate, low-fat diet in type 2 diabetes: A 2-year randomized clinical trial [randomized trial; moderate evidence]
Davis et al. (2009) compared a 33% carb, 23% protein diet to a 50% carb, 19% protein diet. Weight loss and improvements to HbA1c were similar for both groups.
Diabetes Care 2009: Comparative study of the effects of a 1-year dietary intervention of a low-carbohydrate diet versus a low-fat diet on weight and glycemic control in type 2 diabetes [randomized trial; moderate evidence]
Brinkworth et al. (2004) compared a recommendation for a 30% protein, 40% carb, and 30% fat diet to a recommendation for a 15% protein, 55% carb, and 30% fat diet. What the subjects actually ate was not reported. No differences in weight loss or HbA1c were found.
Diabetologia 2004: Long-term effects of advice to consume a high-protein, low-fat diet, rather than a conventional weight-loss diet, in obese adults with type 2 diabetes: one-year follow-up of a randomised trial [randomized trial; moderate evidence]
Pedersen et al. (2013) compared a 30% protein, 30% fat, and 40% carb diet to a 20% protein, 30% fat, and 50% carb diet. There were no differences in weight loss or HbA1c at 12 months.
Nutrition, Metabolism, and Cardiovascular Disease 2014: High protein weight loss diets in obese subjects with type 2 diabetes mellitus [randomized trial; moderate evidence]
Larsen et al. (2011) compared a diet of 42% carb and 26% protein to a diet with 48% carbs and 19% protein. There were no differences in weight loss or HbA1c between groups.
Diabetologia 2011: The effect of high-protein, low-carbohydrate diets in the treatment of type 2 diabetes: a 12 month randomised controlled trial [randomized trial; moderate evidence]
Gardner et al. (2018) (DIETFITS) compared a “healthy low carb” group to a “healthy low fat” group. The “healthy low carb” group ate, on average, 132 grams of carbs and 93 grams of protein daily. The “healthy low fat” group ate, on average, 212 grams of carbs and 84 grams of protein daily. There was no weight loss difference between groups at 12 months.
JAMA 2018: Effect of low-fat vs low-carbohydrate diet on 12-month weight loss in overweight adults and the association with genotype pattern or insulin secretion: the DIETFITS randomized clinical trial [randomized trial; moderate evidence]
Yancy et al. (2010) compared a diet with 62 grams of carbs and 112 grams of protein to a group that ate 186 grams of carbs and 78 grams of protein and took the weight loss drug orlistat. Although only the low-carb group showed a reduction in HbA1c compared to baseline, there was no significant difference in HbA1c between groups, nor was there any difference in weight loss.
Archives of Internal Medicine 2010: A randomized trial of a low-carbohydrate diet vs orlistat plus a low-fat diet for weight loss [randomized trial; moderate evidence]
Increased protein and better outcomes with low-carb: 13 studies
Yancy et al. (2004) compared a diet with 8% carbs and 26% protein to a diet with 52% carbs and 19% protein. The low-carb diet group lost more weight and body fat mass and had lower triglycerides.7
Annals of Internal Medicine 2004: A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: a randomized, controlled trial [randomized trial; moderate evidence]
Jonsson et al. (2009) compared a paleo diet with 32% carbs (125 grams) and 24% protein (94 grams) to an ADA diet with 42% carbs (196 grams) and 20% protein (90 grams). At the end of the study, the paleo group had better weight loss, lower HbA1c, and improved waist circumference compared to the ADA diet group.
Cardiovascular Diabetology 2009: Beneficial effects of a Paleolithic diet on cardiovascular risk factors in type 2 diabetes: a randomized cross-over pilot study [randomized trial; moderate evidence]
Westman et al. (2008) compared a diet with 13% carbs and 28% protein to a low glycemic index diet with 44% carbs and 20% protein. The low-carb group had better weight loss, HbA1c reduction, and diabetes medication reduction.
Nutrition and Metabolism 2008: The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus [randomized trial; moderate evidence]
Saslow et al. (2014) compared a diet with 57 grams of carbs and 105 grams of protein to a diet with 138 grams of carbs and 67 grams of protein. The low-carb group had better HbA1c reduction.
PLoS One 2014: A randomized pilot trial of a moderate carbohydrate diet compared to a very low carbohydrate diet in overweight or obese individuals with type 2 diabetes mellitus or prediabetes [randomized trial; moderate evidence]
Tay et al. (2014) compared a diet with 14% carbs and 28% protein to an energy-matched diet with 53% carbs and 17% protein. Improvements in HbA1c and blood sugar fluctuations were greater in the low-carb group. The two diet groups had equal weight loss.
Diabetes Care 2014: A very low-carbohydrate, low-saturated fat diet for type 2 diabetes management: a randomized trial [randomized trial; moderate evidence]
Yamada et al. (2014) compared a diet with 126 grams of carbs and 100 grams of protein to a diet with 203 grams of carbs and 68 grams of protein. The low-carb group had better HbA1c reduction.
Internal Medicine 2014: A non-calorie-restricted low-carbohydrate diet is effective as an alternative therapy for patients with type 2 diabetes [randomized trial; moderate evidence]
Daly et al. (2006) compared a diet with 34% carbs (110 grams) and 26% protein to a diet with 45% carbs (169 grams) and 21% protein. The low-carb group had better weight loss; there were no significant differences in HbA1c at three months.
Diabetes Medicine 2006: Short-term effects of severe dietary carbohydrate-restriction advice in Type 2 diabetes–a randomized controlled trial [randomized trial; moderate evidence]
Samaha et al. (2003) compared a diet with 37% carbs and 22% protein to a diet with 51% carbs and 16% protein. The low-carb group had better weight loss and more improvement in insulin resistance.
NEJM 2003: A low-carbohydrate as compared with a low-fat diet in severe obesity [randomized trial; moderate evidence]
Shai et al. (2008) compared a low-fat diet with 51% carbs and 19% protein to both a Mediterranean diet with 50% carbs and 19% protein and a “low-carb” diet with 40% carbs and 22% protein. The low-carb and Mediterranean diet groups had better weight loss than the low-fat diet group.
NEJM 2008: Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet [randomized trial; moderate evidence]
Chen et al. (2020) compared a diet with 88 grams of carbs and 82 grams of protein to an ADA diet with 151 grams of carbs and 72 grams of protein. The lower-carb group had better A1c, weight loss, waist circumference and blood pressure. There was no difference in CIMT.
PLoS One 2020: Effect of a 90 g/day low-carbohydrate diet on glycaemic control, small, dense low-density lipoprotein and carotid intima-media thickness in type 2 diabetic patients: An 18-month randomised controlled trial [randomized trial; moderate evidence]
Luger et al. (2013) compared a diet with 38% carbs and 26% protein to a diet with 50% carbs and 17% protein. The lower-carb group had greater reductions in fasting glucose, body mass index (BMI), and insulin requirements.
Experimental and Clinical Endocrinology and Diabetes 2013: Feasibility and efficacy of an isocaloric high-protein vs. standard diet on insulin requirement, body weight and metabolic parameters in patients with type 2 diabetes on insulin therapy [randomized trial; moderate evidence]
Volek et al. (2009) compared a diet with 12% carbs (45 grams) and 28% protein (105 grams) to a diet with 56% carbs (208 grams) and 20% protein (72 grams). The lower-carb group had better weight loss and blood sugar levels.
Lipids 2009: Carbohydrate restriction has a more favorable impact on the metabolic syndrome than a low fat diet [randomized trial; moderate evidence]
Gardner et al. (2007) compared four diets: An Atkins diet with 35% carbs and 21% protein; a Zone diet with 45% carbs and 20% protein; a LEARN diet with 47% carbs and 19% protein; and an Ornish diet with 52% carb and 18% protein. The Atkins group had better weight loss than all others at 2 and 6 months, while that difference was only maintained at 12 months against Zone. Fasting glucose and insulin levels were not different among groups.
JAMA 2007: Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial [randomized trial; moderate evidence]
Summary
As you can see, we do not get the complete picture when we say, “low-carb diets increase weight loss and reduce blood sugars as well as – or significantly better than – higher carb diets.” Instead, it is more accurate to say, “low-carb, higher protein diets increase weight loss and reduce blood sugars as well as – or significantly better than – higher carb, lower protein diets.”While reducing carbs and increasing protein seem to have independent beneficial effects on certain health parameters, the research shows that combining these two strategies may have an even greater positive impact.
Start your FREE 30-day trial!
Get instant access to healthy low-carb and keto meal plans, fast and easy recipes, weight loss advice from medical experts, and so much more. A healthier life starts now with your free trial!
Start FREE trial!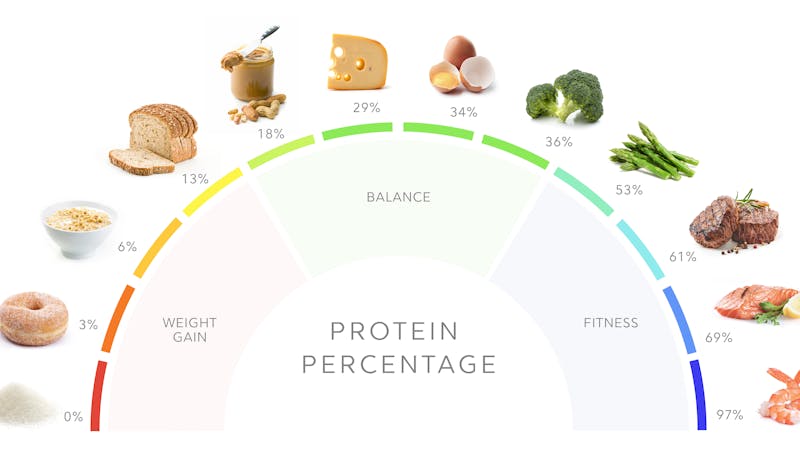


Learn more about protein
- MEMBERS ONLY
![Why more protein is better]()
![Too much protein is better than too little]()
![Why you shouldn't fear protein on keto]()
- MEMBERS ONLY
![Is fear of protein the new fear of fat?]()
- MEMBERS ONLY
![Insulin, protein and how to slow aging]()

Low-carb studies broken down by protein content - the evidence
This guide is written by Dr. Bret Scher, MD and was last updated on August 5, 2022. It was medically reviewed by Dr. Michael Tamber, MD on August 5, 2022.
The guide contains scientific references. You can find these in the notes throughout the text, and click the links to read the peer-reviewed scientific papers. When appropriate we include a grading of the strength of the evidence, with a link to our policy on this. Our evidence-based guides are updated at least once per year to reflect and reference the latest science on the topic.
All our evidence-based health guides are written or reviewed by medical doctors who are experts on the topic. To stay unbiased we show no ads, sell no physical products, and take no money from the industry. We're fully funded by the people, via an optional membership. Most information at Diet Doctor is free forever.
Read more about our policies and work with evidence-based guides, nutritional controversies, our editorial team, and our medical review board.
Should you find any inaccuracy in this guide, please email andreas@dietdoctor.com.
Even when protein content is similar, it is still possible that a low-carb diet will outperform a higher carb diet with respect to naturally reducing caloric intake without trying. This may be because some types of carbs are known to stimulate cravings, keeping calories higher on a higher carb diet. It’s also possible that ketones – often produced by burning fat stores on a low-carb diet – directly suppress appetite. ↩
This result isn’t too surprising, given that participants in the higher carb group ate fewer carbs than prescribed, and participants in the lower carb group ate more than prescribed, making the ultimate difference between carb intakes very small. ↩
These researchers were testing the following diets: high-carbohydrate, high-glycemic-index; high-carbohydrate, low-glycemic-index; and low-carbohydrate, high-monounsaturated-fat. ↩
This result isn’t too surprising, given that participants in the higher carb group ate fewer carbs than prescribed, and participants in the lower carb group ate more than prescribed, making the ultimate difference between carb intakes very small. ↩
The Atkins group ate 85 grams of carbs, while the ADA group ate 208 grams. Caloric intake was not significantly different. ↩
The low-carb group was prescribed 20% of energy from carbs but ate 31%. ↩
Compared to the low-carb group, more people in the low-fat group dropped out of the trial; the authors infer this was probably due to dissatisfaction with the diet and/or the amount of weight loss. The authors did use a statistical tool that analyzed all enrolled subjects in order to account for the different dropout rates.
It’s also important to note that only the low-carb group received supplements from the study’s sponsor (Atkins), including a multivitamin, low-dose fish oil blend, and a “dietary supplement.” None of the ingredients in any of the supplements would be likely to contribute substantially to weight loss. Nonetheless, the authors rightly note that they cannot distinguish effects of the different diets from effects of the supplements. ↩